



Multiple Dermal Ulcers in a Case od Feline Nocardial Mycetoma
Abstract
A 4 month old unneutered male cat was presented at the Veterinary Teaching Hospital of Iasi, with severe dermal lacerations on the posterior side of the right thigh, up to the last rib of the right hemithorax and opened fracture of the right femoral proximal epiphysis, wounds induced by a profound dog bite. The cat underwent reconstructive surgery of the femoral fracture and dermal laceration, full recovery lasting up to three weeks. After the complete healing of lesions, four weeks later, the cat was presented again for consultation, presenting multiple dermal ulcers developing rapidly over 24h on the left thigh, at the marginal limit of the initial dermal laceration. The owner did not report any other changes in the general state of the cat. Physical examination revealed indurated masses of the subcutaneous tissues, with pockets containing reddish-brown exudate. Cytological examination of exudate sampled from a superficial sight of the formation indicated a granular proteic fond, with numerous neutrophils and macrophages. Cytological and microbiological diagnosis was performed on samples collected from a profound sight of the subcutaneous pockets. Microbiological tests isolated and identified Nocardia spp. as pathogen. The exact nocardial species will be further confirmed by polymerase chain reaction analysis and gene sequencing. Antimicrobial drug of choice in this case was erythromycin, administered parenterally for ten days and continued by oral therapy up to 12 months to prevent relapse.
Key words: dermal ulcers, feline nocardiosis, Nocardia spp, nocardial mycetoma.
Introduction
Nocardia spp. (order Actinomycetales, family Nocardiaceae) is filamentous branching gram-positive bacteria (Carp-Carare, 2014), found as ubiquitous soil saprophyte. Until present, almost 50 species of Nocardia have been recognized. Approximately half of these species have been observed to be pathogenic in both human and veterinary medicine. As an opportunistic bacterium, Nocardia is developing with predilection in hosts with an impaired immune system. Nocardia spp. infections are acquired by inoculation by puncture wounds and inhalation of organisms from the environment. Transfer of infection between animals or transmission from diseased animals to humans has not been demonstrated until present (Sykes, 2014). However, nocardiosis has been reported in humans with profound scratch or bite wounds from healthy cats or dogs. Differential diagnosis should include actinomycosis, streptomycosis, mycobacteriosis, bartonellosis, fungal infections, neoplasia and/or leishmaniosis.
Nocardiosis in felines can be presented in pulmonary, systemic, and solitary extrapulmonary forms. In some cases pulmonary nodules, masses and/or effusion can cause cough and tachypnea. Neurologic signs, chorioretinitis, abdominal effusion are indicators of signs of dissemination. Most often reported systemic clinical signs include lethargy, weight loss and inappetence. Systemic disease is reported to be secondary to primary cutaneous-subcutaneous lesions. Cutaneous-subcutaneous infections are described as mycetomas (Rinaldi, et al. 1983), abscesses or cellulites with draining sinuses, develop after scratch or bite wounds. The lesions are usually presented as subcutaneous masses and non-healing, crusted or draining lesions (Praveen, et al. 2011, Farias, et al. 2012).
General characteristic of affected individuals reported until present include 80% male gender, with no predilection for any breed, all ages can be affected and case history usually includes underlying disorders. The epidemiology of feline nocardiosis has been reported worldwide in a hand full of studies (Table 1) (Malik, et al. 2006, Sykes, 2014), with no cohort reports until present in Romania.
Table 1. Nocardia species isolated in cats (Sykes, 2014).{Sykes, 2014 #355;Sykes, 2014 #355}
| Nocardia Species Isolated in Cats with Nocardiosis | |
| N. nova
N. cyriacigeorgica N. africana N. elegans N. brasiliensis N. otitidiscaviarum N. tenerifensis |
United States, Australia
Australia Japan, Brazil Japan United States Spain |
The current study reveals a case of nocardial mycetoma in a cat, most probably appeared after inoculation of the pathogen via a dog bite wound and/or direct exposure of the wound to soil.
MATERIALS AND METHODS
Case report
A four month old male entire Domestic Short Hair cat was presented at the Veterinary Teaching Hospital with dermal lacerations on the posterior side of the right thigh, up to the last rib of the right hemithorax and opened fracture of the right femoral proximal epiphysis, wounds induced by a profound dog bite. The cat underwent reconstructive surgery of the femoral fracture and dermal laceration. Postoperative treatment consisted in administration of antibiotic amoxycillin / clavulanic acid (12.5 mg/kg PO q12h) for seven days. Full recovery was obtained in three weeks and the cat was released home in stable conditions. The follow-up of the case indicated normal appetite and activity level. Four weeks later, after release and complete healing of lesions, the cat was brought back to the clinic presenting multiple dermal ulcers developed over 24h at the marginal limit of the initial dermal laceration (Figure 1). Musculoskeletal system indicated unwillingness/inability to properly use the left posterior limb, and indurated masses of the subcutaneous tissues, with pockets containing reddish-brown exudate were observed.

Figure 1. Cutaneous-subcutaneous lesion developed over 48h, with nodular and indurated subcutaneous tissue.
General physical examination revealed a body temperature of 38.2°C, heart rate of 180 beats per minute, a respiratory rate of 55/min, pink mucous membranes, well hydrated, a normal appetite and a BCS of 3/5. No additional clinically significant abnormalities were present in other systems.
RESULTS AND DISCUSSIONS
Laboratory findings
Haematological and general biochemistry
Complete blood count abnormalities consisted of neutrophilic leukocytosis with a left shift, monocytosis, but with no abnormalities of the red blood cells. Serum general biochemistry of the present case indicated marked phosphataemia of 9.8 mg/dl (range reference: 4-7.3mg/dl) with no other alterations observed.
Plain radiological imaging
Radiographs of the left posterior limb revealed soft tissue swelling, without bone lysis and/or periosteal proliferation. Pulmonary radiography did not indicate the presence of nodules, intra/extra pulmonary masses or bronchointerstitial to alveolar infiltrates, nor any other lesions (Vulpe, 2006).
Microbiologic diagnosis
Superficial cytological examination of the exudate indicated a granular proteic fond, with numerous degenerate neutrophils and macrophages. Micro-granule samples collected from a profound sight of the subcutaneous pockets, were examined crushed between slides (Rapuntean, 2005) with Gram colorations and Fite-Faraco modification of the Ziehl-Neelsen technique, decolorized with 1% sulphuric (Greene, 2006). Observed microscopic morphologic characteristics were described as gram positive, acid resistant, thin branched filaments, with a diameter of 0.5 to 1 µm (Figure 2) (Rapuntean, 2005). Subsequent smears performed from a series of subcultures obtained on solid media did not reveal acid resistance (Greene, 2006).
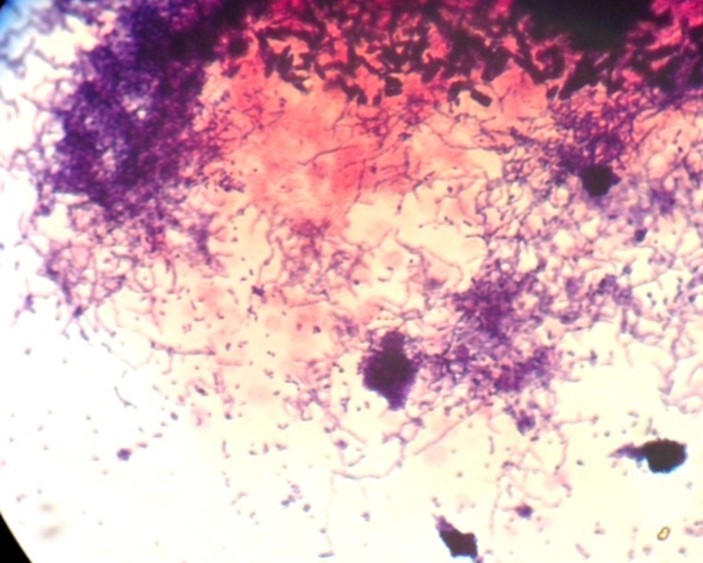
Figure 2. Gram positive branched filaments, col Gram x100
Cultural characteristics were highlighted on blood agar, incubated at 37°C. Type R colonies, with white powdery appearance and firm adherence to the media surface were observed on 48h cultures (Figure 3) (Rapuntean, 2005).
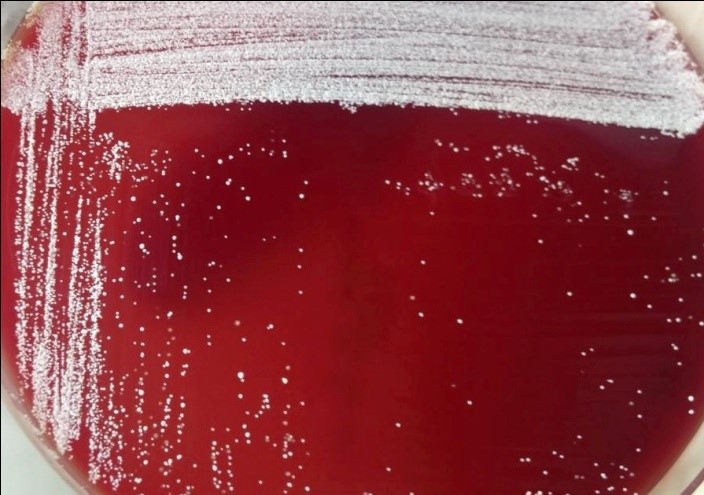
Figure 3. White powdery appearance on blood agar 48h
The powdery appearances of colonies were given by the aerial hyphae (Figure 4).
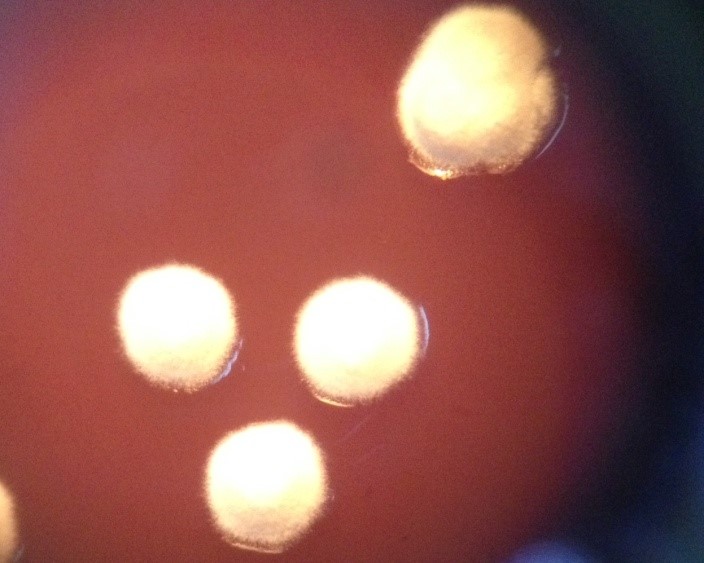
Figure 4. Nocardial colonies, aerial hyphae observed on stereomicroscope x40.
Subcultures were obtained from the first culture, by transferee to Sabouraud (Figure 5) and Lowenstein media.

Figure 5. Sabouraud media, Nocardia cultures at 21 days.
The diagnosis for Nocardiosis has been established based on the morphological and cultural characters of the isolate. Differential diagnosis for Nocardia, from other Actinomycosis has been established based on the time required for culture growth (starting with 24h in Actinomyces, >48h in Nocardia) gram-positive stain, partially acid-fast using Ziehl-Neelsen – Fite-Faraco modified technique, compared to Actinomyces which stains non-acid-fast, the presence of aerial hyphae (not observed in Gordonia, Rhodococcus and/or Tsukamurella) (Murray, et al. 2003).
For the present case, the nocardial species will be further confirmed by polymerase chain reaction analysis and gene sequencing.
Treatment
The susceptibility to antibiotics indicated enrofloxacin and erythromycin as first choice treatment agents. The cat was started on 5 mg/kg/24h of parenterally enrofloxacin, but on the fourth day of administration no improvements have been observed and dermal ulcerations were progressing rapidly.
The second antimicrobial drug of choice was erythromycin, administered parenterally 20mg/kg/24h for ten days and continued by oral therapy, 10 mg/kg bid recommended for 6 months.
After ten weeks of antibiotic administration an attempt for relapse was observed, presented as dermal erosions on the same sight as the initial mycetoma. The antibiotic dose has been increased to 20 mg/kg/12h and the duration for treatment has been extended to 12 months. Cutaneous erosions disappeared when antibiotic dose has been increased and the cat underwent full recovery (Figure 6).

Figure 6. Full recovery of the cutaneous/subcutaneous nocardiosis on 20mg/kg/12h of erythromycin.
The high dose of antibiotic and the long duration of treatment were motivated by nocardiosis relapse, the risk for systemic dissemination and the high mortality (up to 44%) associated with Nocardia spp in cats (Sykes, 2014). In most cases, nocardiosis treatment requires a combination of appropriate antimicrobial drugs, as indicated by the susceptibility test. Treatment duration can be extended on a period of time ranging from 1 to 6 months in cats with cutaneous/subcutaneous form. Individuals diagnosed with the pulmonary or systemic form of the disease, or with underlying immunosuppressive disorders should follow an imperative prolonged treatment protocol reaching to 12 months of antibiotic administration.
CONCLUSIONS
The key for the diagnosis was the sampling of pathogenic material from a profound sight of the subcutaneous pockets. Microbiological tests and cultures on different media provided all information for Nocardia spp diagnosis. Although susceptibility test indicated enrofloxacin as a first choice treatment agent, clinical results failed to appear, requiring a second antibiotic selection. Long term treatment should be considered in immunocompromised individuals, with systemic nocardial infections, or as in the present case with relapsing infections. Sustained adequate antibiotherapy is an important aspect of feline Nocardiosis, preventing recurrence and progression to systemic forms of the disease which involve a high mortality.