



Chapter 1: Introduction to the Study
Introduction
Healthcare organizations operate in uncertain times of healthcare reform. Therefore, strong, ethical and professional leadership can guide organizations to act in the best interest of the staff and patients. Ethical culture, with its expected input of virtuousness and emotional wellbeing, can positively enhance outcomes independently of individual employee’s specific value and ethics, as a result, managerial efforts should be heavily focused on creating an ethical culture (Ruiz-Palomine, Martinez-Canas, & Fontrodona, 2013). Improving employee’s perceptions of ethics in the organization, such as fairness, clarity of expectations, accountability, and leadership prioritization, could impact healthcare organizational outcomes (Cohen, Foglia, Kwong, Pearlman & Fox, 2015). In the current health care arena, the level of patient satisfaction depends on clinical leadership and nurses’ ability to communicate effectively during the delivery of care (Moore et al., 2016).
The drive to provide effective communication to the patient stems from new financial sanctions implemented by CMS, which can withhold two percent of hospitals’ inpatient payments (CMS, 2016). The consequence of the new financial sanctions is that acute care hospitals focus on increasing patient satisfaction and organizational performance through improving communication (Mazurenko et al., 2016). Recent studies on hospital communication indicate that an open dialogue between patients and nurses positively influences the patients’ experiences and satisfaction assessments (Ford, Huerta, Diana, Kazley, & Menachemi, 2013). These links between organizational ethical culture and outcome verifies the importance of organizational ethical culture and its impact on productivity and customer satisfaction.
There is very limited empirical research on the relationship between an organizational ethical culture and patient satisfaction in health care organizations. According to Riivari and Lasma, (2014), organizational ethical culture influences innovation and they have concluded that strong ethical culture has a direct impact on organizational culture and innovation. Nevertheless, this study did not include other aspects of an organization’s outcome such as financial outcome, productivity, efficiency, commitment, and work satisfaction. Riivari and Lasma, (2014), recommended further research to include these outcomes. Ethical leadership behavior is related to the perception of ethical climate, and ethical climate mediates the influence of the managers on individual ethical behavior outcome (Demirtas & Akdogan, 2015). However, findings of this study cannot be generalized to other industries and they suggested further research should include other variables and outcomes as counter-production and group level behaviors.
The aim of this research is to address the gap in literature and explore healthcare organizational ethical culture’s impact on patient satisfaction. Improving patient satisfaction and organizational performance has been a challenge for healthcare organizations. In the past, research on organizational ethical culture and performance has yielded limited results on ethical culture influence on the healthcare industry, in particular, its effect on patient satisfaction (Cohen et al., 2015). Hence, when healthcare organizations possess high level of ethical culture they experience less staff turnover, more productivity, increased patient safety, cost effectiveness, and a high level of patient satisfaction. Effective leadership in healthcare is important for the achievement of optimal patient outcomes (Wong, Cummings, & Ducharme, 2013). Recent studies on hospital communication indicate that an open dialogue between patients and nurses positively influences the patients’ experiences and patients’ satisfaction assessments (Ford, Huerta, Diana, Kazley, & Menachemi, 2013). Nursing care has the most substantial impact on the HCAHPS overall rating top-box percentage with measuring patient satisfaction and can have implications on hospitals reimbursements (Wolosin, Ayala, & Fulton, 2012).
There are a number of studies that have identified the relationship between ethical culture, climate and moral distress in healthcare (Atabay et al., 2015; Oh & Gastmans, 2015). Other studies explored the correlation between ethical climate and organizations’ effectiveness including job satisfaction turnover and commitment (Demirtas & Akdogan, 2015; Huang, You &Tsi, 2011; Ebtisam Aly, 2017). However, the proposed study will offer new insight into the application of corporate ethical virtues on patient care delivery and patient satisfaction regarding nursing communication. The findings of this study will contribute to the body of knowledge concerning ethical theory and model, as well as its relationship to patient satisfaction. The specific focus of this study lies in the examination of a relationship between organizational ethical virtues in nursing and patient satisfaction in a large academic hospital.
The researcher will use a quantitative methodology to examine the relationship between nursing ethical culture and patient satisfaction at a large academic center in North East United States. The primary foundation of this study is the Corporate Ethical Virtues (CEV) model as it formulates normative and multi-dimensional measures for evaluating the ethical culture of an organization (Kaptein, 2008). This study seeks to investigate the relationship between nursing ethics as perceived by frontline nursing and patient satisfaction. The researcher will collect data using the corporate ethical virtues model (CEV) to measure ethical culture (Kaptein, 2013), facilitated by using Survey Monkey, a web-based survey tool. The Opinion Meter, which is based on the questions on the Hospital-Consumer Assessment of Healthcare Providers and Systems (HCAHPS; CMS, 2015), will be used to measure patient rating of nurses’ communication during their hospitalization. The Opinion Meter survey will be administered directly to the patient that is assigned to the same nurse (Appendix G).
The remainder of this chapter will focus on the background of the study, statement of the problem, purpose of the study, the proposed research questions and hypotheses, how this research will advance scientific knowledge, and the significance of the study. Moreover, this chapter contains a brief overview of ethical leadership, organization’s ethical culture, patient satisfaction, as well as rationale for using quantitative research methodology and the research design. This chapter will conclude with a list of the definition of terms, assumptions, limitations, delimitations, and a summary organization of the rest of the study.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Introduction This section provides a brief overview of the research focus or problem, explains why this study is worth conducting, and discusses how this study will be completed. (Minimum three to four paragraphs or approximately one page) | ||||
| Dissertation topic is introduced and value of conducting the study is discussed. | 2 | 2 | ||
| Discussion provides an overview of what is contained in the chapter. | 2 | 2 | ||
| Section is written in a way that is well structured; has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: Sound good but see above comments 12/20 . |
Background of the Study
Healthcare organizational ethical culture has a powerful influence on the organization performance because it is manifested in the organization’s climate, behaviors, and strategies that support the organizational goals. The primary responsibilities of healthcare leaders are to ensure that their organization provides the highest quality of care and services. Ethics affect how and why decisions are being made. Personal ethics can affect leadership and organization and should not be compromised. Therefore, leaders must determine and make ethics a priority because it can produce ethical and effective leadership outcome (Ciulla, 2004). Leadership ethics directly and indirectly affects organizational commitment and turnover intention (Demirtas, & Akdogan, 2015). Ethical culture contributes to teamwork, enhances job satisfaction and encourages the accomplishment of the organization’s mission and objective. Therefore, ethical leadership has significant impact on ethical climate and employees’ ethical behavior (Lu &Lin, 2014).
In the Western philosophy, Virtue ethics has been an important part of the concerns of the major philosophers of ancient Greece, most notably Socrates, Plato and Aristotle. A virtue, according to Aristotle (384-322 BCE), isa trait of mind or character that helps us achieve a good life, which Aristotle argued is a life in accordance with reason. . Solomon (1999, 2000, 2004 and Kaptein, 1998, 1999) applied the virtue theory in an organizational context. According to the theory, both individuals and organizations require certain virtues for moral behavior. Solomon (1992), opined that virtues ethics do not impose prohibited principles or rules of business of behaviors. However, it fosters an intrinsic motivation that leads to successful ethical and business behaviors. For decades, in the western world, ethical organizational culture has been focused on work environment to gauge quality of shared values, norms, and beliefs that could stimulate ethical behavior (Kaptein, 2008; Trevino & Weaver, 2003). Ethical culture effectiveness did not depend only on the culture alone, but on the relationship between cultures and the environment where employees are expected to raise above distinguishing between right and wrong and promoting ethical behavior and make ethical decisions (Schein, 2006).
Virtue ethics shift the focus from actions and conducts to agent and character (Kaptein, 2016). Virtues provide useful methods of understanding leadership; they encompass moral qualities that an individual can have only if he or she practices them. Virtues, like traits, are dispositions to behave in certain ways. Unlike traits, however, virtues are intentionally selected, deliberately strengthened and behaviorally predictive (Ciulla, 2013). Ethical organization culture promotes positive outcomes in an organization (Huhtala, Kangas, Lamsa, & Feldt, 2013). Healthcare leaders must understand the value and the importance of delivering an emotionally and behaviorally intelligent leadership style in order to empower their employees for the implementation of quality healthcare delivery (Delmatoff & Lazarus, 2014). Therefore, organizational ethical cultures are important factors of organizational performance and outcome.
The importance of incorporating and soliciting patients’ perspective of healthcare delivery and qualify have been established in the literature. In recent decades, Patient satisfaction has become an important concept for both as a metric for quality care and patient perception of their care. The relationship between patient satisfaction and quality of care has been discussed in the past but without consensus. Dionabedian (1966) divided patient quality of care into two main parts: technical performance and interpersonal relationship which both can be assessed from the patient prospective. Dionabedian (1966) argued that in addition to health status, patient satisfaction is the ultimate outcome of patient care delivery. In healthcare, patient satisfaction become an essential component of patient outcome and care delivery (Dionabedian, 1988). The inaugural quality assurance of Donabedian (1980) identified the importance of patient satisfaction and quality assurance in healthcare. In healthcare, the importance of measuring patient statistics is well discussed (Link & Kelly, 1995), patient satisfaction has been studied and measured exclusively as a stand-alone construct and as an element of quality outcome (Heidegger et al, 2006). In the 1970s and 1980s, hospitals start working on organizational structures and management process in effort to improve patient satisfaction. New initiatives as shared governance, primary nursing, staff involvement and case management become part of the organizational structure and quality of patient care, and it is considered essential to for organizational survival.
Nurses’ ability to communicate effectively with their patient is considered to be one of the most effective ways to increase patient satisfaction. Nursing care is a major component and determine of patient satisfaction with the overall hospital care (Abramowitz, Cote & Berry, 1987). Effective communication between nurse and patient is paramount in establishing the nurse-patient relationship that provides the basis for enhancing patient care and potentially affecting health outcomes (Hogue, 1979; Kasch & Lisnek, 1984). Nurses’ communication with patients is associated with patient satisfaction with care and an indicator of patients’ perception of the quality of nursing care received (Thomas & Bond, 1992). Regulatory and accreditation agencies have established standard requirement for patient satisfaction assessment as part of the continues quality improvement measurement and reporting (JCAHO, 2000). The quality of nurse environment was found to be associated with ten measures of patient satisfaction and strongly related to patient recommending the hospital (Kutney et al, 2009). Patient perception of the quality of nursing communication is more likely to influence overall patient satisfaction score than physicians’ communication (Boulding, Glickman, Manary, Schulman, & Staelin, 2011).
Quality of care and patient satisfaction is considered an essential component of nursing work. Nursing leadership has a central role in meeting the quality agenda (Haycock-Stuart & Kean, 2012). Hospitals with poor nursing work environments have lower patient satisfaction scores than hospital with positive nursing work environment (Brooks- Carthon et al., 2011; Papastavrous et al., 2014).
Furthermore, ethical culture has been found to influence some important employee outcomes such as job satisfaction, behaviors, job performance, employee’s wellbeing and employee trust (Chughtai, 2014; Ogunfowora, 2014; Tu & Lu, 2013; Walumbwa et al., 2011; Xu, Loi, & Nqo, 2016). Hospitals need to be strategical in their plan in order to improve patient satisfaction (Smith, 2014).
There is paucity of research that examines the relationship between organizational ethical culture and patient satisfaction related to nurses’ communication. Ethical culture affects employees’ perception of procedural and distribution justice, which is crucial in fostering justice and trust, and a fair workplace (Xu et al., 2016). Ethical culture impacts different organizational outcomes; therefore, it supports additional research to explore the underlying factors of this relationship (Riivari & Lasma ,2014; Demirtas & Akdogan, 2015; Xu et al., 2016). The review of the literature yielded limited research studies conducted that examine ethical culture impacts on different organizational outcomes; therefore, further research is required to explore the underlying factors of this relationship (Riivari & Lasma ,2014; Demirtas & Akdogan, 2015). According to Riivari and Lasma (2014), organizational ethical culture influences innovation. Nevertheless, this study did not include other aspects of an organization’s outcome such as, financial outcome, productivity, efficiency, commitment and work satisfaction. Riivari and Lasma (2014) recommended further research should include these outcomes. Ethical leadership behavior is related to the perception of ethical climate, and ethical climate mediates the influence of the managers on individual ethical behavioral outcomes (Demirtas & Akdogan, 2015). However, findings that this study unearthed is not all encompassing. Research suggests that other variables and outcomes that will serve as counter-production and group level behaviors should be considered. The aim of the proposed research then, is to address the gap in the literature and explore healthcare organizational ethical culture’s impact on patient satisfaction.
Despite the ongoing research on ethical culture and ethical leadership, little is known about the influence of nursing ethical culture as perceived by frontline staff and its relationship with patient satisfaction related to nursing communication. This study will contribute to health quality outcomes by empirically investigating the relationship between organizational ethical culture as perceived by frontline nursing staff and its effect on patient satisfaction related to nurses’ communication.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Background of the Study The background section explains both the history of and the present state of the problem and research focus. It identifies the “gap” or “need” based on a summary of the current literature and discusses how the study will address that “gap” or “need.” (Minimum two to three paragraphs or approximately one page) | ||||
| Provides a summary of results from the prior empirical research on the topic and identifies the need as defined by the prior research which this current study will address. | 2 | 2 | ||
| Section is written in a way that is well structured; has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Problem Statement
It is not known, what relationship (if any), exists between nursing perception of organizational ethical culture and patient satisfaction related to nurses’ communication, in healthcare organizations. Improving employee’s perceptions of ethics in the organization, such as fairness, clarity of expectations, accountability, and leadership prioritization, could impact healthcare organizational outcomes (Cohen, Foglia, Kwong, Pearlman & Fox, 2015). Healthcare organizations with dysfunctional cultures could result in damaging consequences. With the continued demand of sustainable organization culture that promotes quality outcomes and patient satisfaction, employees’ perception of their ethical leadership culture is essential in establishing the platform for transformation, improvement, and change to meet the demand for quality improvement and patient satisfaction.
The stakes are high for hospitals in the United States to improve patient satisfaction scores. Patient satisfaction is a dynamic concept that can have a huge impact on the hospital. Patient satisfaction scores are important reflection of patient care and should be closely monitored due to the adverse effect of losing Medicare reimbursements and its potential impact on hospital revenue. Several researchers examined employees’ perception of ethical leadership and its impact on job performance (Huhtalas et al., 2012; Neubert & Roberts, 2013; Wong et al., 2013; Demirtas, & Akdogan, 2015; Riivari & Lasma, 2013; Cohen, Foglia, Kwong, Pearlman & Fox, 2015). However, the perception of an organization’s ethical virtues by healthcare employees—using the Corporate Ethical Virtues (CEV) model (Kaptein, 2008)—and its relationship to patient satisfaction related to nursing communication have not been explored, thus resulting in a gap in our knowledge.
This study will focus on the influence of nursing ethical culture on certain organizational outcome in hospital nursing units, with particular emphasis placed on scores of communications with nurses. Accordingly, the unit of analysis is frontline nursing staff and their assigned patients. The study will be limited to frontline nursing staffs with at least one-year clinical experience who are involved in direct patient care in an inpatient hospital setting. Nurses with the registered nurses (RNs) tag will be included while healthcare workers with in the manager or director position will be excluded.
The target population for this study is frontline RNs and their assigned patients on medical and surgical inpatient units at a medical center in New York. The total population is 200 registered nurses (RNs). The sample for this study will include at least 128 RNs and their assigned 128 patients. A quantitative correlational study will be conducted to serve as the research design for this research. The independent variable is the frontline employees’ perceptions of leadership ethics as measured by the eight dimensions of the CEV Model which includes clarity, congruency of supervisor and congruency of management, feasibility, supportability, transparency, discussability, and sanctionability. The dependent variable will be patient satisfaction as measured by the Opinion MeterOpinion Meter which is based on an item from the HCAHPS survey that relates to nurses’ communication with patients.
There is a need to identify the perception of frontline nurses’ on the nursing ethical culture and examine its relationship with patient satisfaction. This knowledge could have practical implications on organizational performance and patient satisfaction. It could also provide specific information and recommendation regarding nursing leadership, communication between nurses and patients, and healthcare organization outcomes.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| States the specific problem proposed for research with a clear declarative statement. Discusses the problem statement in relation to the gap or need in the world, considering such issues as: real issues affecting society, students, or organizations; the frequency that the problem occurs; the extent of human suffering the problem produces, the perceived lack of attention in the past; the discussion of the problem in the literature and research about what should be addressed vis à vis the problem; the negative outcomes the issue addresses. | 2 | 2 | ||
| Describes the general population affected by the problem. The general population refers to all individuals that could be affected by the study problem. Example: All older adults in the US who are 65 years or older. The target population is a more specific sub-population of interest from the general population, such as low income older adults (≥ 65 yrs) in AZ. Thus, the sample is derived from the target population, not from the general one. | 2 | 2 | ||
| Describes the unit of analysis, which is the phenomenon, individuals, group or organization under study. | 2 | 2 | ||
| Discusses the importance, scope, or opportunity for the problem and the importance of addressing the problem. | 2 | 2 | ||
| 2 | 2 | |||
| Section is written in a way that is well structured; has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: See above comments |
Purpose of the Study
The purpose of this correlational study is to investigate the degree of the existent relationship between ethical leadership and patient satisfaction at a healthcare organization in New York City. A quantitative correlational study will serve as the research design for thisstudy. The independent variable in this case will be the frontline nurses’ perceptions of organizational ethics as measured by the eight dimensions of the CEV Model which includes clarity, congruency of supervisor and congruency of management, feasibility, supportability, transparency, discussability, and sanctionability. The dependent variable will be patient satisfaction as measured by the OpinionMeter which will be based on an item from the HCAHPS survey that relates to nurses’ communication with patients.
When healthcare organizations possess high levels of ethical culture, they experience less staff turnover, more productivity, improved patient safety, overall cost effectiveness and higher level of patient satisfaction (Cohen, Foglia, Kwong, Pearlman, & Fox, 2015). Therefore, improved ethics in an organization could have an impact on healthcare organizational outcomes. The independent variable is the organization’s ethical virtues as measured by the RNs perception of ethics using the Corporate Ethical Virtues (CEV) scale (Kaptien, 2008). The CEV model composes eight virtues, which are embedded in the organization’s culture and it represents the ethical quality of the organization culture. The CEV scale dimensions includes clarity, congruency of supervisor and management, feasibility, supportability, transparency, discussability, and sanctionability. The CEV model formulates normative and multi-dimensional measures for evaluating the ethical culture of an organization and provides support for the existence of ethical leadership.
The dependent variable is the outcome of patient satisfaction score of nurses’ communication through the Opinion Meter which will be administered to a patient that is assigned to a corresponding nurse in the unit. The Opinion Meter questionnaire will focus only on nursing communication with a patient, and it is based on questions from the Hospital Consumers Assessment of Healthcare Providers and Systems (HCAHPS; CMS, 2013). Through the Opinion Meter, only one item from the HCAHPS survey which relates to communication with nurses will be administered. The Opinion Meter questionnaire include patients perception through the following questions during their hospital stay: How often didyournurse treat you with good manners and respect? How often did your nurse listen to your concerns? Did your nurse communicate to you in a way you could understand? After you pressed the call button and ask for help, do the nurses respond to you in a timely manner?
RNs demographic variables that includes the respondents’ (Registered nurses) sex (male/female), age (years), education (degree), race, years of service, position in the organization, and shift assigned will be collected.
Frontline nurses are the main professionals in hospital settings who encounter and respond to patients’ needs. The target population are frontline registered nurses with a minimum experience of a year in medical and surgical inpatient units at a medical center in New York. It is important to gather information from frontline employees and also aggregate these individual evaluations in order to gain a better understanding of the shared nature of nursing ethical culture. Nursing is a profession that requires expertise, skills to meet patients’ need and assistance in helping patients deal with problems.
Nursing is a therapeutic approach to patient care. The relationship between the nurse and patient is beneficial and based on trust and mutual understanding, as well as open communication that fosters mutual goal setting (Peplau, 1997). In essence, improved staff communication skills would eventually increase patient satisfaction. According to Oni (2012), the implication of effective communication to the patient can potentially lead to increased patient satisfaction, prevent loss of reimbursement, increase referrals, and ensure a more virtuous status in the community. Improved nurse-patient communication would improve quality care, potentially decrease anxiety, lead to improvement in safety, and enable patients to develop trust in nursing care, all of which potentially may lead to speedy recovery.
The setting for this study will be medical- surgical patient care inpatient units at a large medical center located in a metropolitan area in New York City, New York. The medical center offers a wide range of services and includes a 650-bed capacity, full-service hospital offering trauma, emergency, medical-surgical, critical care, obstetric, pediatric, psychiatry, cardiovascular, and critical care services. The medical center has a base of 5,500 employees, of which 1,040 are staff RNs who work in a variety of settings, such as medical-surgical units, behavior health units, intensive care units, the emergency room, and outpatient services. The hospital employs only few licensed practical nurses (LPNs) and approximately 700 unlicensed support staff which include patient care associates (PCAs), and patient care technicians (PCTs). However, the current study will focus only on the 200 registered nurses (RNs) who only work in the medical surgical units. Other inpatient and outpatient staff will not be included. The patient population included patients from all socioeconomic status within the New York metropolitan area.
The purpose of this quantitative correlational study is to assess the influence of organizational ethical virtues on healthcare quality outcome of patient satisfaction that are related to nurses’ communication. This study is significant because it will help to determine whether a healthcare worker who exhibits certain ethical virtues affects organizational outcomes. The findings from this study could provide specific information and recommendations regarding improvement of healthcare organization outcomes and patient satisfaction.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| PURPOSE OF THE STUDY Minimum two to three paragraphs | ||||
| Begins with one sentence that identifies the research methodology and design, target population, variables (quantitative) or phenomena (qualitative) to be studied and geographic location. This can be presented as a declarative statement: “The purpose of this study is….” that identifies the research methodology and design, population, variables (quantitative) or phenomena (qualitative) to be studied and geographic location. | 2 | 2 | ||
| Describes the target population and geographic location. | 2 | 2 | ||
| Quantitative Studies: Defines the variables and relationship of variables. Qualitative Studies: Describes the nature of the phenomena to be explored. | 2 | 2 | ||
| Section is written in a way that is well structured; has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Research Question(s) and Hypothesis
It is not known what relationship (if any) exists between organizational ethical culture and patient satisfaction in healthcare organizations. Improving employee’s perceptions of ethics in the organization, such as fairness, clarity of expectations, accountability, and leadership prioritization could impact healthcare organizational outcomes (Cohen, Foglia, Kwong, Pearlman & Fox, 2015).Patient care is mostly administered directly and/or indirectly through frontline nursing staff. Therefore, the guiding research questions and hypothesis for this study is the relationship of nursing perceived organizational ethical virtues and patient satisfaction relate to nurses’ communication in nursing units (surgical and medical units) within a large metropolitan hospital.
The independent variable is the organizational ethical virtues as measured by the nurses’ perception of ethics using the Corporate Ethical Virtues (CEV) scale which have eight dimensions of clarity, congruency of supervisor and management, feasibility, supportability, transparency, discussability, and sanctionability. The dependent variable will be the outcome of patient satisfaction score of nurses’ communication through the Opinion MeterOpinion Meter that measures patient perception of communication with nurses. Demographic variables will include RNs demographics data, which include years of experience, level of education, age, sex, race, and the type of nursing unit assigned. Patient care by nursing and communication of nurses are more predictive than interactions with physicians and they are the factors that influence overall patient-experience scores in hospital settings (Manary, Boulding, Staelin, & Glickman, 2013). The variables for this study were selected to address the following research question and hypothesis:
RQ1: Is there is relationship between organizational ethical culture and patients’ rating of communication with nurses?
H1: Organizational ethical culture is positively related to patients’ rating of communication with nurses.
H01: Organizational ethical culture is not related to patients’ rating of communication with nurses.
RQ2: Is there is relationship between the dimension of clarity and patients’ rating of communication with nurses?
H2: Clarity is positively related to patients’ rating of communication with nurses.
H02: Clarity is not related to patients’ rating of communication with nurses.
RQ3: Is there is relationship between the dimension of congruency of supervisor and patients’ ratings of communication with nurses?
H3: Congruency of supervisor is positively related to patients’ rating of communication with nurses.
H03: Congruency of supervisor is not related to patients’ rating of communication with nurses.
RQ4: Is there is relationship between the dimension of congruency of management and patients’ rating of communication with nurses?
H4: Congruency of management is positively related to patients’ rating of communication with nurses.
Ho4: Congruency of management is not related to patients’ rating of communication with nurses.
RQ5: Is there is relationship between the dimension of feasibility and patients’ rating of communication with nurses?
H5: Feasibility is positively related to patients’ rating of communication with nurses
Ho5: Feasibility is not related to patients’ rating of communication with nurses
RQ6: Is there is a relationship between the dimension of supportability and patients’ rating of communication with nurses?
H6: Supportability is positively related to patients’ rating of communication with nurses
Ho6: Supportability is not related to patients’ rating of communication with nurses
RQ7: Is there is a relationship between transparency and patients’ rating of communication with nurses?
H7: Transparency is positively to patients’ rating of communication with nurses
Ho7: Transparency is not related to patients’ rating of communication with nurses
RQ8: Is there is a relationship between the dimension of discussability and patients’ rating of communication with nurses?
H8: Discussability is not related to patients’ rating of communication with nurses.
Ho8: Discussability is positively related to patients’ rating of communication with nurses.
RQ9: Is there is a relationship between the dimension of sanctionability and patients’ rating of communication with nurses?
H9: Sanctionability is positively related to patients’ rating of communication with nurses.
Ho9: Sanctionability is not related to patients’ rating of communication with nurses.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Research Question(s) and/or Hypotheses Minimum two to three paragraphs or approximately one page | ||||
| Qualitative Studies: States the research question(s) the study will answer and describes the phenomenon to be studied. Note: The research questions provide guidance for the data which will be collected to answer the research questions; they do not identify the instruments. Quantitative Studies: States the research questions the study will answer, identifies and describes the variables, and states the hypotheses (predictive statements) using the format appropriate for the specific design and statistical analysis. | 2 | 2 | ||
| This section includes a discussion of the research questions, relating them to the problem statement. The research questions need to be connected to the theory(s) or model(s) from the theoretical foundation section, as well. | 2 | 2 | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
Advancing Scientific Knowledge and Significance of the Study
Nursing leadership ethics influence on patient satisfaction is a study that very few empirical researches have addressed many studies that have been conducted have focused on the relationship between organizational ethical culture and innovativeness (Rivera & Lasma, 2012). Huhtala, Feldt, Hyrone and Maurono’s (2012) study focused on ethical organizational culture and its influence on the working environment and managers’ commitment to organizational goals. According to Hassan (2013), ethical leadership behavior can increase organizational commitment by reducing staff absentees (Shin, Sung, Choi, & Kim, 2015). Ethical leadership has significant influence on employees’ mindset, behavior and commitments (Neubert & Roberts, 2013).
A gap in the literature exists regarding ethical culture impact on organizational outcome of patient experience. Strong associations can be found between ethical leadership and ethical organizational culture, and lower ethical strain, lower burnout and higher work engagement (Huhtula, 2011). Promoting ethical virtues in organizations can lead to a virtuous circle, which supports ethical leadership and ethical culture (Huhtala, Lamsa, & Feidt, 2013). However, limited research is available when investigating the links between leadership ethical virtues and organizational outcome of patient satisfaction. Riivari and Lamsa (2014) investigated the connection between ethical culture and organizational effectiveness from both public and private sector organizations and from all levels of the organizations. Rivera and Lamsa’s (2014) study revealed that there is a relationship between ethical organizational culture and the specific organizational outcome of organizational innovativeness. However, the researchers were not able to study other areas of outcomes such as productivity and efficiency. Therefore, the authors suggested studying other organizational outcomes and its relationship to ethical culture.
The framework of this study builds upon Solomon’s (1992, 1999, 2000, & 2004) ethical virtues theory of business ethics and the Corporate Ethical Virtues (CEV) model, which formulates normative and multi-dimensional measures for evaluating the ethical culture of an organization (Kaptein, 2008). According to Solomon (1999, 2004) and Kaptein (1998), both individuals and organizations should have certain virtues that lead to moral behavior. To date, the CEV model has been used in a small but growing number of studies, indicating, for example, that a strong ethical culture is related to lower levels of unethical behavior (Kaptein, 2011b), ethical leadership (Huhtala, Kangas, Lämsä, & Feldt, 2013), better organizational innovativeness (Riivari, Lämsä, Kujala, & Heiskanen, 2012), and higher number of managers’ personal work goals related to the organization’s success (Huhtala, Feldt, Hyvönen, & Mauno, 2013).
This investigation quantitative study will be conducted in order to examine the relationship between ethical virtues in nursing using the CEV model, and patient satisfaction related to nurses’ communication with patients at a healthcare organization in New York City. The findings of the study can offer further knowledge and understanding of ethical culture within the context of healthcare. This study will provide additional evidence on the importance of the way leadership practices are perceived by frontline employee. The investigation will add to the scientific body of knowledge by providing empirical evidence as to the relationship between nursing ethical virtues and patient satisfaction at a healthcare organization in NYC.
The significance of this study is the contribution to the body of knowledge related to the relationship between organizational ethical virtues and patient satisfaction. Understanding how ethical organizational culture can influence patient outcome has important implications, as this information can be directed towards new and more effective interventions. The study will identify the ethical culture virtues of healthcare leaders based on the Corporate Ethical Virtues (CEV) model (Kaptein, 2008). The model formulates normative and multi-dimensional measures for evaluating the ethical culture of an organization and provides support for the existence of ethical leadership dimension of clarity, congruency of supervisor and management, feasibility, supportability, transparency, discussability, and sanctionability as perceived by frontline nursing staff and its impact on patient satisfaction related to nursing communication. The findings of this research may provide data for organizations to improve their performance through the understanding of leadership ethical culture dimensions, and how they can enhance the creation of strong culture, and promote ethics, empowerment, commitment, and employee satisfaction, which can lead to improved patient satisfaction.
The CEV scale provides managers, other organizational members, and outsiders such as consultants with a practical tool with which to assess ethical organizational culture (Huhtala, 2013). Organizations need to support ethical practices at the work unit level in order to enhance employee engagement while reducing burnout (Huhtala, Tolvanen, Mauno, & Feldt, 2015). The findings of this research can offer a platform to prepare the next generation of nursing leadership. In addition, the findings of this research can offer organizations a potential for a nursing leadership framework for the creation of an ethical environment that can improve and sustain staff and patient satisfaction. The findings of this research also has the potential to enlighten scholars, policy makers, practitioners, recruiters, and other educational stakeholder about nursing ethical influence on frontline employees and organizational outcomes.
Knowledge from this study could be used by organizations to examine their current ethical culture and create cultural changes in health care organizations. In order to examine healthcare organizational performance and patient experience, organizations need to explore and identify the relationship between frontline employees’ perception at their organization and leaders’ ethical culture, and organizational outcome of patient satisfaction. Healthcare organizations monitor patient experiences in order to evaluate and improve the quality of care. Nurses spend a lot of time with patients; they have a major impact on patient experiences (Westbrook, Duffield, & Creswick, 2011). To improve patient satisfaction, nurses need to know what factors within the nursing work environment are of influence. The main focus of this research is to explore nurses’ perception of their organization and leadership ethics and its relationship to their communication with patients, ultimately to explore the relationship between ethics and patient care.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| ADVANCING SCIENTIFIC KNOWLEDGE and SIGNIFICANCE OF THE STUDY (Minimum one to two pages) | ||||
| Clearly identifies the “gap” or “need” in the literature that was used to define the problem statement and develop the research questions. | 2 | 2 | ||
| Describes how the study will address the “gap” or “identified need” defined in the literature and contribute to the body of literature. | 2 | 2 | ||
| Describes how the research fits with and will contribute to or advance the current literature or body of research | 2 | 2 | ||
| Describes the potential practical applications from the research. | 2 | 2 | ||
| Identifies the theory(ies) or model(s) that provide the theoretical foundations or conceptual frameworks for the study. | 2 | 2 | ||
| Connects the study directly to the theory and describes how the study will add or extend the theory or model. | 2 | 2 | ||
| Describes how addressing the problem will add value to the population, community, or society. | 2 | 2 | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Rationale for Methodology
This study will use a quantitative approach to investigate the relationship among nursing ethical virtues and patient satisfaction in a health care organization. Studies of ethical leadership culture have utilized both quantitative and qualitative methods (Brown et al., 2005). Quantitative research seeks to establish relationships between study variables and seeks to clarify a hypothesis through statistical data analysis of numerical data. According to Babbie (2012), a quantitative methodology is ideally suited for the investigation of a relationship between two measurable variables. In the case of this study, quantitative methodology was chosen in an effort to statistically analyze the relationship between nursing ethical culture and patient satisfaction. This allows determining whether the relationship patient satisfaction and nursing perception of organizational ethical virtues in a New York City hospital is significant.
Quantitative research methods attempt to maximize objectivity, replicability, and generalizability of findings, and are typically interested in prediction. Fundamental to this approach is the expectation that a researcher will set aside his or her experiences, perceptions, and biases to ensure objectivity in the conduct of the study and the conclusions that are drawn (Harwell, 2011). A qualitative method would not have been appropriate for this study as qualitative research involves the collection of non-numerical and non-statistical data (Denzin, 2012), and is not ideal for measuring relationships among variables. A qualitative study is more appropriate for collecting subjective data about the experiences of sample participants— which was not the purpose of this research.
Researcher can use quantitative methodology when studying patient population which helps avoid the researcher’s influence, which can occur in qualitative research methodology. Furthermore, qualitative methodology concludes themes instead of examining the relationship between variables.( Mis, 2013). In the proposed study, the second variable is patient satisfaction and the study will attempt to investigate the relationship between two variables; organizational ethical culture and patient satisfaction. Therefore, quantities methodology is appropriate for this study. A mixed-method methodology is utilized in situations where, in addition to analyzing numerical data, the researcher interacts directly with study participants through interviews or direct observation to collect qualitative data (Johnson & Christensen, 2012). Since this study will involve no such interaction, a mixed-method methodology would also be inappropriate.
The body of research on organizational ethical culture is growing. However, there is still need for more theoretical knowledge and empirical findings (Huhtala et al., 2013). In order to improve ethical quality in healthcare organizations, there is a need to examine their overall ethical practices, standard and expectation, alignment and consistency with norms (Pearlman et al., 2013). In Pearlman et al.’s (2013) study, a quantitative research methodology was appropriate for the study for its preciseness in measuring the variable (i.e., dependent, independent, and control variables).
There is no single blueprint for planning research. Research design is governed by the notion of fitness for purpose. The purpose of the research determines the methodology and design of the research (Cohen, Manion, & Morrison, 2011). Quantitative research methods provide strategies to conduct systematic and controlled statistical test to measure and conform hypotheses (Hogan, 2014). Therefore, a quantitative methodology will be conducted to investigate the relationship among organizational ethical virtues and patient satisfaction related to nursing communication at a healthcare organization in New York City. In summary, a quantitative methodology is considered to be the most appropriate approach to addressing the research questions posed in this study.
| Criterion* (Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Rationale for Methodology (Minimum two to three paragraphs) | ||||
| Identifies the specific research methodology for the study. | 2 | 2 | ||
| Justifies the methodology to be used for the study by discussing why it is an appropriate approach for answering the research question(s) and addressing the problem statement. Quantitative Studies: Justify in terms of problem statement and the variables for which data will be collected. Qualitative Studies: Justify in terms of problem statement and phenomenon. | 2 | 2 | ||
| Uses citations from seminal (authoritative) sources (textbooks and/or empirical research literature) to justify the selected methodology. Note: Introductory or survey research textbooks (such as Creswell) are not considered seminal sources. | 2 | 2 | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Nature of the Research Design for the Study
A correlational quantitative study will serve as the research design. One approach to a fuller understanding of human behaviors is to begin by teasing out simple relationships between those factors and elements deemed to have some bearing on the phenomena in question. The value of correlation research is that it is able to achieve this end (Cohen et al., 2011). Researchers use a correlational design when they want to examine the relationships among variables. A correlational study, regardless of the significance of the findings, does not imply causation, but shows a relationship between variables (Polit & Tatano-Beck, 2012). The quantitative correlational design is the most effective method to investigate the relationship among two or more variables; it provides numerical estimates of the relationship with a comparison of the strength of any identified differences between the two or more variables (Cohen et al., 2011). Correlation techniques are generally intended to answer three questions about variables or sets of data. First “Is there a relationship between the variables or set of data? When the answer is “yes” two other questions will follow “what is the direction of the relationship and “what is the magnitude?” (Cohen et al., 2011). A correlational research design will be used for this study because of its ability to measure the degree of association between variables, not which one causes a change in the other (Gay et al., 2011). This study will use a correlational approach to quantify the relationship among the variables in questions. This will also reduce the personal bias often found through the gathering and analysis of qualitative data (Gay et al., 2011). A correlational design is optimal for this study because the objective is to investigate the relationship between organizational ethical virtues and patient satisfaction related to nursing communication.
This study will focus on the influence of nursing perception of organizational ethical culture on patient satisfaction on hospital medical surgical nursing units, in particular, scores of communication with nurses. Accordingly, the unit of analysis will be both the perception of the staff nurses regarding organizational ethical culture and perception of their assigned patients about their satisfaction related to their nurses’ communication. Frontline nursing staff with at least one-year of experience who is involved in direct patient care in an inpatient hospital setting. Nurses with a title of Registered Nurses (RNs) will be included; nurses with a title of manager or director will be excluded.
Determining the size of the sample will also have to take account of attrition and respondent mortality, i.e. that some participants will leave the research or fail to return questionnaires. Hence it is advisable to overestimate rather than to underestimate the size of the sample required. It is clear that sample size is a matter of judgment as well as mathematical precision (Cohen et al., 2011). The size of a probability (random) sample can be determined by using a power analysis via the G*power program. G*Power is a stand-alone power analysis software, used for various statistical tests (Peng, Lomg, & Abaci, 2012). Prior research suggests that a medium size effect is expected in the present research. Thus, the input parameters for one regression model are an adjusted medium effect size of 0.25, an alpha of 0.05, and a power of 0.80, since there are eight dimensions for the CEV. These parameters will result in a computation of a minimum sample size of 128 as the number representative of the total sample size.
Data will be collected through an online survey via Survey Monkey, including basic demographic data which include the following items: (Registered nurses) gender (male/female), age (years), education (degree), race, years of service and primary shift, and the CEV scale of ethical culture. The targeted healthcare organization is a large medical center in New York. It employs approximately 1,040 Registered nurses and the target population is approximately 200 Registered nurses in the medical surgical inpatient units. The sample population for this study will include at least 128 medical- surgical registered nurses with at least one year of experience. In addition, the same numbers of assigned patients will be surveyed for their nurses’ communication. In the medical- surgical units, each nurse usually assigned to at least 6 patients, therefore, a randomized sample of 128 patient will surveyed.
Written permission to access the participants for this research will be obtained from the Internal Review Board (IRB) for the research site. Prior to collection of data, informed consent will be obtained from the participants, and a educational and informational meeting will be conducted with the frontline nursing staff to solicit volounteers. The researcher will initiate a forum to communicate the intent of the study, explain the study procedures, and answer questions.
Multiple linear regressions will be conducted on the data in order to understand relationship among variables. Both descriptive and inferential statistical data will be analyzed to identify relationship and correlations between variables and to answer the research questions. Descriptive statistics will be used to describe the demographics and to determine the summaries and frequency distribution for each variable in the study.
Quantitative data will derive from the demographic questionnaire, CEV scale measurements, and patients’ Option Meter survey scores regarding communication with nurses. The Opinion Meter questionnaire will focus only on nursing communication with a patient, and it is based on the questions from the Hospital Consumers Assessment of Healthcare Providers and Systems (HCAHPS; CMS, 2013). The quantitative method is strong at studying large groups of people and also uses quantifiable numerical data such as frequencies, means, medians, standard deviations, variances, and other statistical procedures for objective observations, assessments and analyses. The dependent variable of communication with nurses will be obtained from the assigned patients through the Option Meter survey scores.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Nature of the Research Design for the Study Minimum three to four paragraphs or approximately one page) | ||||
| Identifies and describes the selected design for the study. | 2 | 2 | ||
| Justifies why the selected design addresses the problem statement and research questions. Quantitative Studies: Justifies the selected design based on the appropriateness of the design to address the research questions and data for each variable. | 2 | 2 | ||
| Briefly describes the target population and sample for the study. | 2 | 2 | ||
| Identifies the sources and instruments that will be used to collect data needed to answer the research questions. | 2 | 2 | ||
| Briefly describes data collection procedures to collect data on the sample. | 2 | 2 | ||
| Describes the unit(s) of observation, which may be individuals, groups, documents, artifacts, databases, based on the data collection plan and instruments/sources. For example, units of observation may be individuals or documents. | 2 | 2 | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Definition of Terms
Health care organizations are known for working within a language unique to the environment. Physicians and nurses use many acronyms and abbreviations, as well as complex medical jargon within the context of written documentation and verbal dialogue. The use of unambiguous and approved list of abbreviations is suggested in order to ensure good communication in patient care (Sinha, McDermott, Srinivas, & Houghton, 2011). The following terms and their operational definition will be used in this study:
Leadership ethics. Refer to the action of behaviors that consist of appropriate norms. It can be defined as the demonstration of normativity appropriate conduct through actions both personal and interpersonal relationship through communication and decision-making (Brown el al., 2005).
Ethical organizational culture. The ethical quality of a work environment that consists of shared values, norms, and beliefs that can stimulation ethical behavior (Kaptein, 2008; Trevino & Weaver, 2003).
Virtue ethics. It is mostly concerned with the intentions, attitudes, qualities, characteristics, and disposition of agent –in other words, the emphasis is on the decision-maker rather than the actions (Crane & Matten, 2007; Kaptein, 2010). The intellectual roots of virtue ethics lie in the work of Plato and Aristotle, which is the basis of the CEV model that will be used in the research to study organizations’ ethical culture.
Patient satisfaction. The degree to which the individual regards a health care service or product, or the manner in which it is delivered by the provider, as useful, effective, or beneficial. Patient satisfaction is a measurement designed to obtain reports or ratings from patients about services received from an organization, hospital, physician or health care provider. Patient satisfaction is a subjective judgment resulting from the appraisal of healthcare experiences and reflects the degree to which an individual’s actual experience matches his or her preferences regarding the experience (Manary, Boulding, Staelin, & Glickman, 2013).
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS). A nationally standardized survey developed by Center for Medicare and Medicaid Services (CMS) and Agency for Healthcare Research and Quality (AHRQ) for measuring how patients perceive the care they receive in hospitals. The survey is the first national standard for collecting patient’s perspectives of care and enabling valid comparisons across hospitals. It was developed to monitor patient satisfaction based on information collected by a questionnaire survey of discharged hospital patients regarding their hospital stay (HCAHPS Fact Sheet, 2015).
Opinion Meter. is a survey tool to measure patient satisfaction scores during their hospital stay. Since this research will focus only on nurses’ communication, therefore, only questions regarding nurses’ communication will be used. The following questions will be administer to patients: How often did the nurse treat you with good manners and respect? How often did your nurse listen to your concerns? Did your nurse communicate to you in a way you could understand her or his explanation? After you pressed the call button and ask for help, Does the nurses responded to you in a timely manner. For this study, the Opinion Meter questionnaire will focus only on nursing communication with patients, The questionnaire is based on the questions from the Hospital Consumers Assessment of Healthcare Providers and Systems (HCAHPS; CMS, 2013).
Centers of Medicare and Medicaid (CMS). An agency within the U.S. Department of Health & Human Services responsible for administration of several key federal health care programs (CMS, 2010).
The Patient Protection and Affordable Care Act of 2010 (PPACA). This act advocates that “healthcare is a right, not a privilege.” The main goals of PPACA are to minimize the number of uninsured Americans and make healthcare available to everyone at an affordable price. One of the greatest benefits of the PPACA is that insurance companies have been prohibited from denying coverage to children based on preexisting conditions. In addition to that benefit, insurance companies are also prohibited from rescinding coverage, and any act of discrimination against adults with preexisting conditions was prohibited in 2014. The most significant provision of the PPACA is that it will provide coverage for the currently uninsured through various methods without further increasing the cost of healthcare (Huntington, Covington, Center, Covington, & Manchikanti, 2011).
Frontline staff. Frontline is a visible forefront in any action, activity, or field. The term frontline nursing staff describes health care workers that provide routine and essential service healthcare environment. Frontline nursing staff mostly includes Registered nurses (RNs). Registered nurses responsibilities includes performing physical exams and health histories, provide health promotion, counseling and education, administer medications, wound care, and numerous other personalized interventions, interpret patient information and make critical decisions about needed actions, coordinate care, in collaboration with a wide array of healthcare professionals, direct and supervise care delivered by other healthcare personnel like LPNs and nurse aides, conduct research in support of improved practice and patient outcomes (ANA, 2017).
Press Ganey Associates. A recognized leader in improving the patient experience for nearly 30 years, Press Ganey partnered with more than 2 6,000 health care organizations across the continuum of care — including 50 percent of all U.S. hospitals — to advance quality of care and stakeholder satisfaction, and ultimately, improve the overall patient experience. The company offers a comprehensive portfolio of solutions that capture the patient voice and identify more targeted improvement opportunities through advanced analytics and strategic advisory services. Press Ganey works with clients from across the continuum of care such as hospitals, medical practices, home care agencies and other providers, The company mission is to help health care organizations reduce patient suffering and enhance caregiver resilience to improve the safety, quality, and experience of care (Press Ganey Associates, 2016).
| Criterion* (Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Definitions of Terms (Each definition may be a few sentences to a paragraph.) | ||||
| Defines any words that may be unknown to a lay person (words with unusual or ambiguous meanings or technical terms) from the research or literature. | 2 | |||
| Defines the variables for a quantitative study or the phenomena for a qualitative study from the research or literature. | 2 | |||
| Definitions are supported with citations from scholarly sources. | 2 | |||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | |||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Assumptions, Limitations, Delimitations
Assumptions are underlying factors that are somewhat out of the researcher control, however if these assumptions disappeared, the study becomes irrelevant (Simon, 2011).The following assumptions will be presented in the study:
- The result of this study can benefit healthcare organizations recognize that the ethics of their nursing culture can influence healthcare organizations outcome of patient experience. The study may also offer insight about nursing leaders’ ability to understand their ethical virtues.
- The finding of this research can provide support to previous research argument for positive effect of an ethical organizational culture on organizational outcome.
- The research will open new avenues in investigating the relationship between ethical culture and healthcare organizational outcome. Quantitative and qualitative as well empirical studies are needed to affirm the role of ethical culture in promoting organizational innovativeness (Riivari, Lämsä, Kujala, & Heiskanen, 2012).
- The frontline nursing perception of ethical organization and leaders’ virtues may assist nursing leadership and organization to focus on these virtues that impact patient satisfaction.
- The assumption that the study participants will answer the survey questionnaire truthfully and to the best of their ability and understanding.
- The corporate ethical virtues (CEV) scale is reliable and valid. The CEV scale can be utilized as a tool to create a better working environment with less ethical strain, less emotional exhaustion and more work engagement (Huhtala, Feldt, Lämsä, Mauno, & Kinnunen, 2011). The Opinion MeterOpinion Meter is a tool based on the HCAHPS survey and it reliable and valid.
- It was assumed that patient satisfaction as reported by Opinion MeterOpinion Meter was an accurate representation of the patient’s satisfaction with hospital care.
Limitation within a study are weaknesses an factors of design or methodology that gathered but the researcher was not able to control which could have effect on the results and the finding of the research (Simon, 2011). The following limitations will be presented in the study:
- One of the limitations is that study will be conducted only in one healthcare organization in one location. The scope of the study will be limited to leadership ethical behaviors and organizational ethical culture as perceived by registered nurses in a local healthcare organization. The study may have limited generalizability to other private or for profit organizations.
- The participants will complete the survey right after the end of work scheduled which may impact their level of response.
- The survey response will be limited to one time data point in 2018. The correctional design of the study can be seen as limitation. The finding of the study can provide mainly knowledge about the relationship between ethical culture and patient satisfaction. From this perspective, a longitudinal research design would be useful to study causality between two phenomena. Hence, it will make it possible to study the relationship overtime.
- The researcher is a leader and employee of the hospital where the research will be conducted. Therefore, the researcher will take steps to ensure participants’ anonymity and data confidentiality.
- The limitations of the Opinion Meter are the languages in which the survey is available. However, there is a translation phone next to each patient which will be used as needed.
Delimitations is the selections and boundaries that established by the researcher which mostly mentioning the items that in control of the researcher and will not be included (Simon, 2011). The following delimitations will be presented in this study:
- The research will only take into account the perspective of a specific group of frontline employee who is registered nurses. The study only took into account the viewpoint of a registered nurse that held no leadership position at a healthcare organization. Other frontline staff, such as support staff, was not included. Furthermore, leaders such as nursing managers and supervisors were excluded from the study.
- This study was intentionally confined to Kaptein’s (2008) model of corporate ethical virtues and through the Opinion Meter, one item from the HCAHPS survey which relates to nursing: communication with patient. There may have been other factors attributes not mentioned or examined in this study that could have contributed to patient satisfaction.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Assumptions, Limitations, and Delimitations (Minimum three to four paragraphs) | ||||
| Provides a definition of the terms: assumptions, limitations, assumption, limitation and delimitations at the beginning of each section. | 2 | 2 | ||
| States the assumptions being accepted for the study (methodological, theoretical, and topic-specific). Provides a rationale for each assumption. | 2 | 2 | ||
| Identifies limitations of the research method, design sampling strategy, data collection approach, instruments and data analysis. Provides a rationale for each limitation. Discusses associated consequences for the generalizability and applicability of the findings. | 2 | 2 | ||
| Identifies delimitations of the research design and associated consequences for the generalizability and applicability of the findings. Provides a rationale for each delimitation. | 2 | 2 | ||
| The section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Summary and Organization of the Remainder of the Study
Chapter 1 provides the description of the study of organizational ethical culture impact on patient satisfaction in healthcare organizations. The background of the study indicates that organizational ethical have an impact on employee attitudes and can increase organizational commitment (Hassan, 2013). The problem statement points out the gap in the literature regarding organizational ethical culture in healthcare and its impact on organizational outcome of patient satisfaction.
Chapter 1 continued to outline the purpose of this quantitative research which is to investigate the relationship among nursing ethical virtues, as perceived by frontline nursing staff, and patient satisfaction related to nursing communication at a healthcare organization in New York City. The rational for the study centered on the thesis that organizational ethics impact organizational outcomes. Hence, it can assist organizations in creating healthy environments that can produce better outcome of patient satisfaction The significant of the study mainly on the possibly that healthcare organizations benefit from knowledge gained and study outcome to improve organizational productivity and sustainability. Chapter 1 highlighted the quantitative research, which is based on the corporate ethical virtues (CEV) model (Kaptein, 2008). The independent variable is the organizational ethical virtues and the dependent variable will be the outcome of patient satisfaction score of nurses’ communication. A correlational quantitative study will serve as the research design. The targeted healthcare organization is a large medical center in New York. Quantitative data will derive from the demographic questionnaire, CEV scale measurements, and Option Meter survey scores regarding communication with nurses. The Opinion Meter questionnaire will focus only on nursing communication with a patient, definition of terms and assumptions, limitations, and delimitations of study presented in the end of chapter 1.
The remainder of this study will follow: Chapter 2 will focus upon three main areas: 1) leadership ethics and concomitant ethical leadership theories, 2) ethical leadership within the organization, and 3) the ultimate impact of ethical leadership on patient satisfaction. The theoretical foundation of the study will be based upon Solomon’s (1992, 1999, 2000, 2004) ethical virtues theory of business ethics and the Corporate Ethical Virtues (CEV) model.
Chapter 3 includes discussion on the type of research within the study and the research methodology chosen. Chapter 4 includes the data collection, analysis process, and results of the study. A summary of the study, conclusion and recommendation for future research will be included in chapter 5.
| Criterion* (Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Chapter 1 Summary and Organization of the remainder of the study (Minimum one to two pages) | ||||
| Summarizes key points presented in Chapter 1. | 2 | |||
| Provides citations from scholarly sources to support key points. | 2 | |||
| Describes the remaining Chapters and provides a transition discussion to Chapter 2. For proposal only, a timeline for completing the research and dissertation is provided. | 2 | |||
| The chapter is correctly formatted to dissertation template using the Word Style Tool and APA standards. Writing is free of mechanical errors. | 2 | |||
| All research presented in the chapter is scholarly, topic-related, and obtained from highly respected academic, professional, original sources. In-text citations are accurate, correctly cited, and included in the reference page according to APA standards. | 2 | |||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | |||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Chapter 2: Literature Review
Introduction to the Chapter and Background to the Problem
The purpose of this study is to explore the extent to which organizational ethics affect patient satisfaction particularly within nursing in a healthcare organization located in a major metropolitan area. The literature review examines current knowledge regarding the relationship between ethical culture and organizational outcomes. This particular review of the literature focuses upon three main areas: 1) leadership ethics and concomitant ethical leadership theories, 2) ethical leadership within the organization, and 3) the ultimate impact of ethical leadership on patient satisfaction. There are numerous studies related to ethical leadership impact on an organization. However, the studies related to ethical culture in healthcare is lacking. Moreover, the results of the literature review revealed insufficient research that examines the relationship between ethical virtues and patient satisfaction related to nurses’ communication.
The researcher conducted a comprehensive search using Grand Canyon University’s Library Research and Resources System. The databases searched included ProQuest Central, academic searches such as EBSCO, ERIC, and Google Scholar. The researcher used search terms and combinations such as ethics, leadership ethics, ethical leadership ethics theories, healthcare organization, and patient satisfaction.
The remainder of this study in this chapter will explore the background to the Problem. The theoretical foundation of the study will be based upon Solomon’s (1992, 1999, 2000, 2004) ethical virtues theory of business ethics and the Corporate Ethical Virtues (CEV) model (Kaptein, 2008).This section will include a subsection of organizational culture, ethical leadership, business ethics, virtue ethics, and patient satisfaction. The review of the literature will focus upon three main areas: 1) leadership ethics and concomitant ethical leadership theories, 2) ethical leadership within the organization, and 3) the ultimate impact of ethical culture on patient satisfaction. Methodology and instrumentation will be explored and a summary will conclude the chapter.
Background to the Problem
Despite the continued research on ethical culture and ethical leadership, little is known about the influence of organizational ethical culture as perceived by frontline staff and its relationship with patient satisfaction related to nursing communication. The purpose of this quantitative, correlational study is to investigate whether a relationship exists between organizational ethical virtues and patient satisfaction related to nurses’ communication with patients. Nurses are the primary, frontline employees in healthcare, and are important in healthcare delivery. Nursing care have the most substantial impact on the HCAHPS overall rating (Wolosin, Ayala, &Fulton, 2012). Therefore, nurses’ perceptions of organizational ethical culture may be an important factor in the ultimate provision of quality patient care.
Researchers have viewed ethical organizational culture for decade through ethical virtues. However, in the Western philosophy, Virtue ethics have a long history and it has been an important part of the concerns of the major philosopher of ancient Greece, most notably Socrates, Plato and Aristotle. A virtue, according to Aristotle (384-322 BCE), is an excellence and it is a way of getting along with others, a way of manifesting in one’s own thoughts, feeling and actions the ideals that aims the entire community. The most important element of an established culture remains adherence to ethics, including the basic rules that hold society together and protect it from degradation (Solomon, 2004). Solomon (2004) developed a theoretical teamwork approach to business for corporations and organizations in general. It is based on Aristotle virtue ethic (1954) which still remains the model of virtue ethics where one has to think of oneself as a member of the larger community and the way to strive to excel to bring what is the best in us and our shared enterprise. Therefore, we can no longer accept the moral idea that “business is business” (Solomon, 2004).
The Aristotelian approach to business ethics emphasizes that individual’s virtue and integrity are the main concepts and that good corporate and social policy encourages and nourishes individual virtues and integrity. According to Solomon (2004), the important aspect of the Aristotelian approach is the emphasis on the vitality of the community and the business conducted within the larger community of humanity. The Aristotelian ethic relies upon virtues which focus on the integrity of individuals and their aggregate cooperation. A virtue has its place in human society. The practice of collective virtue is essential in order to bind individuals to the larger human network (Solomon, 2004). Integrity within a corporate business includes the virtues of loyalty, congeniality, cooperation and trustworthiness (Solomon, 2004). Hence, the corporation itself needs to be viewed as a morally and socially responsible agent. According to Solomon (2004), the corporation is neither a legalistic fiction nor a financial power in and of itself. Such entities are reflective of their people and communities working together for common goals. Solomon (1999, 2000, 2004 and Kaptein, 1998, 1999) applied the virtue theory in an organizational context. Kaptein (2008) approaches ethical organizational culture through ethical virtues. According to the theory, both individuals and organizations require certain virtues for moral behavior. According to Solomon (1992), virtues ethics do not impose prohibit principles or rules of business of behaviors. However, it fosters an intrinsic motivation that leads to successful ethical and business behaviors.
Ethical organizational culture is an ethical quality of the work environment that consists of shared values, norms, and beliefs that can stimulate ethical behavior (Kaptein, 2008; Trevino & Weaver, 2003). Benner (1997) stated that although the care ethic is foundational to nursing, virtue ethics are enmeshed in care, and nurses should practice from a comprehensive moral philosophy. In the category of virtue ethics, a moral course of action is decided upon based on virtues of character, traditionally including justice, beneficence, non-maleficence, and autonomy, which are four key values underlying the ANA (2001) Code of Ethics. Virtue ethics arises from the work of Aristotle and underlies much the proposed research study bout virtues ethics related to patient satisfaction.
Organizational culture and its values and ethics are key constructs in the healthcare delivery and the adaption of the emerging trend. The trends in healthcare indicate that patients are becoming a consumer’s savvy who are chasing healthcare services that include a balance between psychosocial and medical needs (Brown & Gallant, 2006). These consumers have developed an expectation of quality care. Therefore, the healthcare industries shifted the focus on patient satisfaction and emphasize the patients’ perception of their care. Due to the emphasis on patient satisfaction, leadership style and capabilities which inspire, motivate and deliver tools that help them provide quality to patients. Since the Late 1990s, patient satisfaction has become an increasingly important factor on healthcare delivery. The importance of incorporating and soliciting patients’ perspective of healthcare delivery and qualify have been established in the literature. In recent decades, Patient satisfaction has become an important concept for both as a metric for quality care and patient perception of their care. The inaugural quality assurance of Donabedian (1980) identified the importance of patient satisfaction and quality assurance in healthcare. In healthcare, the importance of measuring patient statistics is well discussed (Link & Kelly, 1995), patient satisfaction has been studied and measured exclusively as a stand-alone construct and as an element of quality outcome (Heidegger et al, 2006). In the 1970s and 1980s, hospitals start working on organizational structures and management process in effort to improve patient satisfaction. New initiatives as shared governance, primary nursing, staff involvement and case management become part of the organizational structure and quality of patient care, and it is considered essential to for organizational survival.
Patient satisfaction is designed to measure patient perception and expectations against the service received (Gallan, Jarvis, Brown & Bitner, 2013). In the U.S nurse compose the Largest group of healthcare professionals and the frontline of patient care in the hospital (Braggiotti, 2012). Leadership have significant role in creating an environment and they are key in influencing the work environment (Lewis & Cunningham, 2016). The quality of nurse environment was found to be associated with ten measures of patient satisfaction and strongly related to patient recommending the hospital (Kutney et al, 2009). The importance of nurse-patient relational communication has been documented through its association with patient satisfaction and perception of quality care, as well as the delivery of cost-effective care (DiMattero, Hayes, & Prince, 1986; Korsch & Negrete, 1981; Thomas & Bond, 1996). Specifically, Fosbinder(1994) found that patients were satisfied with a nurse who took charge of a situation, appeared to enjoy her work, provided information and explanations, and remained friendly. Evidence also exists that poor communication by nurses costs the health system money, may lead to poor nurse performance, and may diminish patient outcomes (Naish, 1996; Tate, 1996).
Healthcare leaders continue to seek ways to improve patient quality, safety, and satisfaction. The Center for Medicare and Medicaid Services (CMS, 2013) for the implementation of Value Based Purchasing (VBP), tied hospital reimbursement to qualify care metric which includes patient satisfaction. Both hospital leadership and frontline nurses play a major role on promoting patient satisfaction. Thus, when healthcare organizations focus on creating ethical climate, such activities tend to improve nursing performance and patient care satisfaction (Greenslande & Jimieson, 2011). Furthermore, nurses comprise the largest group of employees within the hospital setting. Therefore, effective nursing leadership is an essential element in the provision of quality healthcare outcomes. Patient satisfaction in health organizations is an important component of organizational achievement and performance. Thus, the Center for Medicare and Medicare Services (CMS) reimbursement standards placed emphasis on the quality of care in general and patient perceptions of their care experiences in particular (CMS, 2013). The new healthcare reform act and the requirements of the Center for Medicare and Medicare Services (CMS) for organizational quality improvement have shifted the emphasis of most healthcare delivery programs from a volume to a value orientation. In order to improve organizational performance and quality, entities must evaluate factors that can impact patients’ perceptions of care. Organizational performance measurements related to services, activities and processes can contribute to the improvement of patient satisfaction and quality care (Koné Péfoyo & Wodchis, 2013).
Ethical organizational culture is an ethical quality of the work environment that consists of shared values, norms, and beliefs that can stimulate ethical behavior (Kaptein, 2008; Trevino & Weaver, 2003). Huhtala, Feldt, Hyvonen and Mauno (2012) concluded that an ethical organizational culture promotes a working environment conducive to the enhancement of internal employee well-being. However, there is very limited empirical research on the relationship between an ethical culture and patient satisfaction in health care organizations. Riivari and Lasma (2013) have concluded that strong ethical leadership has a direct impact on organizational culture and innovativeness. Nevertheless, this study did not include other aspects of an organization’s outcome, namely employee morale and financial solvency and correlation to patient satisfaction.
Ethical leadership is an important aspect of creating virtuous climates in which both nursing and patient outcomes can be enhanced (Markarott, Storch, Pauly, & Newton, 2014). Professionals invoke specific moral assumptions. Healthcare professionals’ morality should be embedded in policies, customer service and practices (Deherty & Purtilo, 2015). When managers apply ethical leadership style through demonstrations of fairness, power sharing, ethical guidance, role clarification and integrity in their behavior and action, employees become more trusting and organizational commitment can increase (Nastiezaie, Bamer, & Salajage, 2016).
The ethical work climate can affect the moral content of an organization. Ethical leaders can empower their followers to follow ethical practices and encourage them in making ethical decisions that prioritize moral social values, and the collective interest of the organization (Choi, Ulla, & Kwak, 2015). Leaders in healthcare bear many ethical responsibilities, including but not limited to integrity, humility, knowledge and understanding of their role. When healthcare organizations possess high levels of ethical culture, they experience less staff turnover, more productivity, and better levels of patient safety, cost savings, and a higher degree of patient satisfaction. Therefore, improving employee’s perceptions of ethics in the organization, such as fairness, clarity of expectations, accountability, and leadership prioritization, could impact healthcare organizational outcomes (Cohen, Foglia, Kwong, Pearlman & Fox, 2015).
Healthcare organizational ethical culture has a powerful influence on organizational performance because it is manifested climate behavior, and strategies that support the organizations mission, vision and goals. Many studies have shown that ethical leadership directly influences follower attitude and behavior in the work environment (Yidong & Xinxin, 2013; Neubert,Wu, & Roberts, 2013;Schaubroeck et al., 2012 ;Kacmar, Carlson, & Harris, 2013). Ethical leadership affects employees’ perception of procedural and distribution justice, which is crucial in fostering justice and trust, and a fair workplace (Xu et al., 2016). Ethical culture impacts different organizational outcomes; therefore, it requires further research to explore the underlying factors of this relationship (Riivari & Lasma ,2014; Demirtas & Akdogan, 2015; Xu et al., 2016). There are a number of studies that have identified the relationship between ethical culture and climate and moral distress in healthcare (Atabay et al., 2015; Oh & Gastmans, 2015). Other studies explored the correlation between ethical climate and organizations effectiveness including job satisfaction, turnover, and commitment (Demirtas & Akdogan, 2015; Huang, You & Tsi, 2011; Ebtisam Aly, 2017). Ethical climate also been correlated to perception of job satisfaction and medical error among Korean nurses (Hwang & Park 2014).
According to Riivari and Lasma (2014) organizational ethical culture influences innovativeness and they have concluded that strong ethical culture has a direct impact on organizational culture and innovativeness. Nevertheless, this study did not include other aspects of an organization’s outcome as, financial outcome, productivity, efficiency, commitment and work satisfaction, Riivari and Lasma (2014) recommended further research to include theses outcomes. Ethical leadership behavior is related to the perception of ethical climate, and ethical climate mediates the influence of the managers on individual ethical behavior outcome (Demirtas & Akdogan, 2015). However, the finding of this study cannot be generalized to other industry and they suggested further research to include other variables and outcomes as counter-production and group level behaviors. The aim of this research is to address the gap in the literature and explore healthcare organizational ethical culture’s impact on patient satisfaction. The proposed study will offer new insight into the application of corporate ethical virtues on patient care delivery and patient satisfaction regarding nursing communication. The study findings will contribute to the body of knowledge concerning ethical theory and model and its relationship to patient satisfaction. The specific focus of this study lies in the examination of a relationship between organizational ethical virtues in nursing and patient satisfaction in a large academic hospital.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| CHAPTER 2 INTRODUCTION (TO THE CHAPTER) AND BACKGROUND (TO THE PROBLEM) This section describes the overall topic to be investigated, outlines the approach taken for the literature review, and argues the evolution of the problem based on the “gap” or “need” defined in the literature from its origination to its current form. (Minimum two to three pages) | ||||
| Introduction: Provides an orienting paragraph so the reader knows what the literature review will address. | 2 | 2 | X | |
| Introduction: Describes how the chapter will be organized (including the specific sections and subsections). | 2 | 2 | X | |
| Introduction: Describes how the literature was surveyed so the reader can evaluate thoroughness of the review. This includes search terms and databases used. | 2 | 2 | X | |
| Background: Discusses how the problem has evolved historically into its current form. | 2 | X | ||
| Background: Describes the “gap” or “need” defined in the current literature and how it leads to the creation of the topic and problem statement for the study. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | X | |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Theoretical Foundations and/or conceptual framework
In this study, the researcher will examine the relationship between nursing perception of organizational ethical culture and its effect on patient satisfaction in health care organization. The framework of this study builds upon Solomon’s (1992, 1999, 2000, and 2004) Ethical Virtues Theory of Business Ethics and the Corporate Ethical Virtues (CEV) model, which formulates normative and multi-dimensional measures for evaluating the ethical culture of an organization (Kaptein, 2008). Solomon’s (1992) ethics and business theory focuses on individuals and business organizations that need to possess characteristics which are virtues in order to excel morally.
Organizational culture. Leaders and managers of organizations and societies are creators, producers, and victims of their own culture. Therefore, one of the unique functions of a leader is not only to create culture standards in a new group, but also to manage subsequent cultural issues which inevitably arise (Schein, 2009). Culture consists of powerful, implicit, and often unconscious forces determining both individual and collective behavior through perception, patterns and values (Schein, 2009). According to Schein (2009), culture is the product of social learning, ways of thinking and behaviors that are shared and become tacit assumptions and elements of success (Schein, 2009).
Ethical culture refers to the ethical quality of the work environment, which is defined as shared values, norms, and beliefs that can stimulate ethical behavior (Kaptein, 2008; Trevino & Weaver, 2003). Ethical culture includes existing conditions that guide organizations to be compliant with ethical expectations. Ethically behaving leaders can develop the culture of his or her organization towards more ethical practices (Huhtala, Kangan, lamsa, & Feldt, 2013).
Ethical leadership. Ethical principles relate to the nature of human wellbeing (Kraut, 2014). Ethical culture encompasses the experience, presumptions, and expectations of the promotion of cultural values (Trevino & Weaver, 2003). Ethical leadership is defined as the behavior of appropriate conduct through personal action and interpersonal relationships (Yang, 2013). According to Brown and Trevino (2006) ethical leadership comprises two different aspects; the moral person and the moral manager. The moral person aspect relates to the leader’s personality that includes their moral characteristic and traits which manifested in their personal and professional life. The moral manager aspect refers to the leader’s intentional effort and concrete actions to influence and guide follower’s ethical behavior. Leadership is distinctive in that moral failure at the upper levels can impact a large number of people (Ciulla, 2012). When leaders act fairly and consider others, employees’ attitude and behavior can be positively affected (Brown & Trevino, 2006). The influence of ethical leadership directly impacts immediate followers, and indirectly ripples across hierarchical levels and culture (Schaubroeck et al., 2012).
Brown, Trevino and Harrison (2005) defined ethical leadership as the demonstration of normatively appropriate conduct through personal action and interpersonal relationship, and the promotion of such conduct to followers through two-way communication, reinforcement, and decision-making. According to Ciulla (2012), an ethical and effective leader is one who does the right thing, the right way, and for the right reasons. Leadership ethics directly and indirectly affect organizational commitment and staff turnover (Demirtas & Akdogan, 2015). Leaders have the power to monitor, motivate, and shape organizational culture by influencing staff behavior and corporate practice based upon the ultimate mission of the organization. Ethical cultures contribute to teamwork, enhance job satisfaction and encourage the accomplishment of the organization’s mission and objective (Lu & Lin, 2014). Ethical leadership includes behaviors such as being trustworthy, inclusive, and fair. Such character traits are imbued in individuals who abide by an appropriate, societal moral compass (Brown & Trevino, 2006).
Virtue ethics. A virtue according to Aristotle is excellence. The Greek word “arête” is often translated to virtue of excellence. Virtue is a state of character, and in order to develop virtuous characteristics one must form certain habits by engaging in the right kinds of activities (Lebowitz, 2013). Aristotle followed both Socrates and Plato in describing virtues as central elements necessary for well-being and a decent life. According to Aristotle, being virtuous is a character or disposition that contributes to happiness or well-being (Ross, 2013). Aristotle classified virtues into intellectual categories that include practical wisdom and deliberative excellence. Secondary virtues around morality encompass justice, liberty, courage and temperance, among others (Richard, 2014). The doctrine of the mean is the central concept of Aristotle’s ethical virtues arguments (Richard, 2014). According to Aristotle, excellent virtues (including personal thoughts and feelings) are an exemplary means of getting along with others, and for dealing with the entire community.
Ethics is not a set of prohibitive principles or rules. Rather, the ethics of virtue are an intrinsic part and driving force of successful life styles (Solomon, 1992). Virtue ethics has a long pedigree, going back to Plato and Aristotle and many others. The virtue is a short-hand way of summarizing the ideals that define good character (Solomon, 1992). Most Aristotle’s virtues are recognizable as business ethics because business is a social activity that involves dealing with other people in both stressful and friendly situations (Solomon, 1992). There are many virtues that are associated with business life as honesty, loyalty, sincerity, courage, reliability, trustworthiness, benevolence, cooperativeness, modesty, openness, sensitivity, decency, reasonableness, persistence, helpfulness, gratefulness, tolerance, warmth and hospitality (Solomon, 1992).
The Corporate Ethical Virtue model (CEV). The CEV model is based on Aristotelian virtue approach which was applied to business ethics by Solomon (1992, 2004). This approach emphasizes individual integrity which needs to be supported by good organizational social policies and practices. The CEV model is grounded in the virtue-based theory of business ethics. Corporate ethical virtue is the organization’s condition of ethical behavior (Kaptein, 2015). The decency of an organization is situational based upon the manner in which employees are stimulated to behave ethically and the barriers which are established to prevent them from behaving unethically (Kaptein, 1998). Therefore, when organizations stimulate employees to behave ethically, virtue increases across the entire entity. According to Solomon (1999, 2004) and Kaptein (1998), both individuals and organizations should have certain virtues which lead to moral behavior.
The CEV model includes eight virtues which are based on existing theories and empirical research which includes a quantitative analysis of 150 cases of unethical behavior (Kaptein, 1998) and validated by four studies (Kaptein, 2008). The virtues include clarity of ethical standards that are concrete, comprehensive and with understandable expectation. Congruency refers to ethical role modelling of supervisors and senior management which reflects managerial behavior. Feasibility refers to the ability to behave ethically that includes the available resources from ethical actions, sufficient time, equipment, financial resources, information and the support and authority to act according to the norms and values. Supportability refers to shared commitment to ethical behaviors through fairness and mutual trust. Transparency refers to the organizational member perception of unethical behavior, and consequences of these behaviors. Discussability refers to the opportunity to raise and discuss ethical issues in order to reduce ethical dilemmas. Finally, the virtue of Sanctionability refers to the likelihood of rewarding employees and managers for ethical behavior and punishment for unethical behavior. (Kaptein, 2008).
To date, the CEV model has been used in a small but growing number of studies, indicating, for example, that a strong ethical culture is related to lower levels of unethical behavior (Kaptein, 2011b), ethical leadership (Huhtala, Kangas, Lämsä, & Feldt, 2013), better organizational innovativeness (Riivari, Lämsä, Kujala, & Heiskanen, 2012), positive correlation between managers’ personal work goals and organization’s success (Huhtala, Feldt, Hyvönen, & Mauno, 2013), and more willingness among managers and employees to report unethical behavior (Kaptein, 2011a).
Patient satisfaction. The Accountable Care Organization (ACO) model and Medicare Shared Saving Program (MSSP) was launched by CMS as an alternative payment approach in order to engage healthcare professionals to assume collective responsibility for the cost and quality outcomes of specific patient populations. The Fee For Services (FFS) Medicare model was designed to further serve beneficiaries (CMS, 2012). Patient satisfaction is one aspect of the quality of care based upon the patient’s perception of healthcare delivery during a hospital stay. Patient satisfaction is related to the quality of care services and is further influenced by the level of trustfulness of the medical and nursing staff (Burcen, Toma, & Pupuc, 2011). Therefore, measuring patient satisfaction is one way to guide operational decisions, which can yield results related to retention of current patients, attracting new ones, and stream-lining nursing practice workflow.
Patient satisfaction reviews are performed by utilizing the Hospitals Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey format. The HCAHPS survey is the first national, standardized, publicly reported survey of patient perspectives of hospital care. This HCAHPS survey is usually sent to recently-discharged patients regarding their hospital stay and healthcare delivery experience. This survey touches upon qualities of healthcare such as compassion and concern, and the responsiveness of the healthcare professional to patient needs and concerns. Furthermore, the Center of Medicare and Medicaid Services (CMS, 2013) ties hospital reimbursement to various quality metrics, including patient ratings of their care experience as measured by the HCAHPS. This type of survey provides hospitals with incentives to emphasize quality care and to enhance the patient experience.
The issue of ethics in business is a global problem. The challenges facing healthcare requires strong leadership. The healthcare industry is unique because it depends upon human beings caring for one another. Thus, patient care is dependent on healthcare professionals. Therefore, the importance of aligning the working environment through collaboration, cooperation, and setting of ethical standards directly empowers leadership and healthcare professionals to provide patients with the highest of quality care. When healthcare organization possess high level of ethical culture, they experience less staff turnovers, more productivity, better level of patient safety, cost saving and high level of patient satisfaction (Cohen, Foglia, Kwong, Pearlman, & Fox, 2015). Therefore, improving employee’s perceptions of ethics in the organization could have impact on healthcare organizational outcome.
In the literature review, the CEV model applied to some studies (Kaptein, 2008, 2009, 2010, 2011, 2015; Solomon & Hanson, 1985; Solomon, 1992, 2004; Riivari et al., 2012; Huhtala et al., 2013; Huhtala et al., 2011; Huhtala, 2013; Huhtala et al., 2015; Kangas et al., 2014).The ethical culture of the organization will be measure with the CEV questionnaire (Kaptein, 2008) the structure of the CEV scale for measuring and evaluation ethical culture has been previously tested and validated by researchers (Kaptein, 2008; Huhtala et al., 2011; Riivari et al., 2012). The background variables (Gender, age, education and position) had significant correlations with some of the CEV dimensions. Therefore, the study will also use these variables and nursing years of service.
The main research question that will guide this study is whether a relationship exsist between nursing perception of organizational ethical virtues in surgical and medical units, and patient satisfaction in a large medical center in New York City. The purpose of this quantitative correlational study is to assess the influence of organizational ethical virtues on healthcare quality outcome of patient satisfaction that related to nurses’ communication. The independent variable is the organization ethical virtues as measured by the RNs perception of ethics using the Corporate Ethical Virtues (CEV) scale (Kaptien, 2008). The dependent variable is the outcome of patient satisfaction score of nurses’ communication through the Opinion Meter which will be administered to a patient that is assigned to a corresponding nurse on the unit.
.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| theoretical foundations and/or conceptual framework This section identifies the theory(ies) or model(s) that provide the foundation for the research. This section should present the theory(ies) or models(s) and explain how the problem under investigation relates to the theory(ies) or model(s). The theory(ies) or models(s) guide the research questions and justify what is being measured (variables) as well as how those variables are related (quantitative) or the phenomena being investigated (qualitative). (Minimum two to three pages) | ||||
| Identifies a model(s) or theory(ies) from seminal source(s) that provide a reasonable conceptual framework or theoretical foundation to use in developing the research questions, identifying variables/phenomena, and selecting data collection instruments. | 2 | 2 | X | |
| Accurately cites the appropriate seminal source(s) for each theory or model. | 2 | 2 | X | |
| Includes a cogent discussion/synthesis of the theory or model and justifies the theoretical foundation/framework as relevant to the study. Connects the study directly to the theory and describes how the study will add or extend the theory or model. | 2 | 2 | X | |
| Builds a logical argument of how the research questions directly align to the theoretical foundation for the study. | 2 | 2 | X | |
| Reflects a deep understanding of the foundational, historical, research relevant to the theoretical foundation/framework. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | X | |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Review of the Literature
Previous research has been conducted on the effect of organizational and leadership ethical culture on organization outcome. However, a paucity of research focused on organizational ethical virtues impact on patient satisfaction related to nurses’ communication, and the gap still exists in determining the relationship between the two variables. The review of the literature will be presented in 6 subsections. The first subsection of this literature review will discuss ethical culture definitions and theories. Next, ethical leadership and organization, ethical virtue and organizations outcome which mostly based on the CEV model (Kaptein, 2008). The next subsection will review research that investigating the impact of ethical culture on patient outcome, nurse work environment, and patient satisfaction. The next subsection will include the concept of patient satisfaction and perception of care and review the existing literature on this topic. The final two subsections will explore different methodology and instrumentation of prior research on ethical leadership, ethical organization and patient satisfaction. Finally, the chapter will be concluded with a summary.
Ethical leadership. Ethical leadership must be perceived as fair, honest, and trustworthy. True leaders must be capable of demonstrating ethical behavior on both a personal and professional level. An ethical leader accomplishes and exhibits moral influence by actively attempting to persuade followers to adopt appropriate ethical behavior. This task is usually accomplished via ethically-oriented communication centered upon value-oriented messages and acting as a role model. Contemporaneously, proper leaders utilize a system of reward and punishment to hold each individual accountable for their own ethical behaviors (Brown & Trevino, 2006). Ethical leaders are expected to behave morally. Leaders must be virtuous while demonstrating strong, moral character (Aristotle, 2011; Solomon, 1992). Moral character is a multidimensional concept consistent with the variation of an individual’s personality traits, one’s self-reputation and moral identity (Cohen, Panter, Turan, Morse, & Kim, 2014).
For leaders to be perceived ethical and influence ethics-related outcome, they need to be perceived as attractive, credible, and legitimate. Based on social learning theory (Bandura, 1986), Jordan, Brown, Trevino, and Finkelstein (2013) proposed that followers’ perceptions of ethical leadership depend on the executive leader’s cognitive moral development (CMD).The authors examined the direct association between the leader’s cognitive moral development, the followers’ perception of ethical leadership, the relationship between leaders and followers’ cognitive moral development and the followers’ perception of ethical leadership.
In order to maximize a follower’s perception of ethical leadership, leaders’ needs to focus upon advanced ethical reasoning and cognitive moral development. Direct reports’ perceptions of ethical leadership were stronger when leaders exhibited higher, cognitive moral development (Jordan et al., 2013). In addition, strengthening cognitive moral development was associated with stronger followers’ perceptions of ethical leadership, when leaders’ cognitive moral developmental was higher than their followers. Hence, executives can increase perceptions of their ethical leadership by distinguishing themselves from followers and by being noticed by their followers with respect to behavioral dimensions based upon explicit communication regarding ethics and ethical conduct. However, Jordan et al. (2013) were not able to determine causality in the relationship between cognitive moral development divergence and perceptions of ethical leadership. Another limitation in this study was the small sample size that restricted the researcher from investigating several important questions and variables. For example, the study did not investigate the relationship between ethical leadership and lower organizational levels. The proposed research on ethical leadership impact on patient satisfaction will focus on the lower organization level which is the nursing frontline staff.
Ethical environments can influence employee’s behavior and practices. Zu, Trevino, and Zheng (2016) found that a leader’s moral identity and moral attentiveness are associated with followers’ perceptions of ethical leadership behavior patterns. Additionally, ethical leadership influences corporate moral identity and moral attentiveness. According to Brown and Trevino (2006), ethical leadership exists on two levels: the moral person and the moral manager. Hence, these two factors lead to a unique approach in transforming a manager’s morality into active promotion of ethical conduct by his or her followers. Explicit communication of ethical expectations and behaviors results in reward and/or punishment (Trevino & Brown, 2007). Therefore, in order to be perceived as ethical leaders, these pillars, around which a leader’s moral compass revolves, are essential in creating ethical environments that influences employee’s behavior and practices. In the proposed research, the author will examine the relationship between ethical leadership and its influence in nurses communication with patients.
According to Ciulla (2013) there are various types of leadership values. These include ethical virtues such as sobriety, chastity, abstention, kindness, altruism, other commandments and rules of personal conduct. Ethical values include honesty, integrity, trustworthiness, reliability, moral value, liberty, security, equality, justice, and community. Each of these types of leadership values has implications on leadership styles, practices and strategies. Moral values are not only standards of measuring our character, transactions, policies, and programs, but also constitute transitional forces that contain evocative and revitalizing ideas for which individuals fight and die (Ciulla, 2013). Leaders cannot empower people unless they have the moral courage to be honest and sincere in their intention to change the power relationship that they have with their followers (Ciulla, 2013). When hiring or promoting within the organization, the supervisory staff must exhibit the characteristics of integrity and honesty, while adhering to the organization’s code of ethics and organizational culture (Wright, 2013).
According to ethical leadership theory, leaders influence follower’s ethical decisions and actions through social learning and exchange processes, communication of ethical standards, and the use of performance management systems for employee conduct and accountability (Brown & Trevino, 2006). A two-stage model was developed and tested by Steinbauer, Renn, Taylor, and Njoroge (2012) to explain how ethical leadership relates to followers’ ethical judgments in an organizational context. Drawing from social learning theory, the researchers investigated followers’ perceived accountability as a linking mechanism between ethical leadership and followers’ self-leadership as focused on ethics. Thus, they argue that a follower’s self-leadership, focused on ethics, is a behavioral manifestation of the follower’s perceived accountability and social learning process. Taken together these factors explain how ethical leadership influences followers ethical conduct. In addition, the study investigated the relationship between ethical leadership and followers ethical decisions.
Self-leadership is the process of leading, motivating and controlling ones overt behavior in order to achieve self-defined goals. The research found that ethical leadership is positively related to followers’ self-leadership focused on ethics. Furthermore, a follower’s perception of his responsibility fully accounted for this leadership. In addition, the study revealed that followers’ self-leadership based ethics were positively associated with followers’ ethical decision-making only when they employed deliberative approaches to decision-making. In addition, the study provided support for the notion that deliberate application of self-leadership, with a focus on ethics, leads to higher moral judgment. These findings provide support for the important of leadership ethics on different type of leadership as self-leadership.
Drawing from social learning and moral identity theories, Mayer, Aquino, Greenbaum, and Kuenzi (2012) conducted two studies. In their first study, they examined the antecedents and consequences of ethical leadership. In their second research, they empirically examined the uniqueness of ethical leadership constructs as compared to related leadership paradigms. These concepts include idealized influence, interpersonal justice, and informational justice. The first study revealed a positive relationship between ethical leadership a leader’s moral identity symbolization, and moral identity internalization. Negative relationships were found between ethical leadership, unethical behavior and relationship conflict. In the second study, a leaders’ moral identity was positively related to ethical leadership, idealized influence, interpersonal justice, and international justice. Ethical leadership was negatively related to unit outcomes. In both studies, ethical leadership partially mediates the effects of a leaders’ moral identity.
According to Mayer et al. (2012), ethical leadership matters when leaders emulate desired ethical behavior, and use rewards and punishment to reinforce ethical behavior. Under such circumstances, employees are less likely to engage in unethical behavior and practices. Therefore, leaders can play an important role in reducing negative outcomes. Leaders set the ethical tone of the organization and are instrumental in encouraging ethical behavior while reducing interpersonal conflict among their subordinates.
Okam and Akyuz (2011) examined the impact of ethical leadership behavior on an employee’s intrinsic and extrinsic job satisfaction. These researchers also examined the effect of loyalty to supervisors. The research analysis revealed that ethical leadership is effective in driving supervisor loyalty and increases job satisfaction. In addition, ethical leadership has a significant, positive correlation with both intrinsic and extrinsic job satisfaction. Due to the limited sampling size of the study, the authors suggested further studies to include inclusion of cultural variables and wider, more extensive samples.
Drawing from social learning theory Brown et al. (2005) found that direct reports’ perceptions of ethical leadership were stronger when leaders exhibited higher, cognitive moral development. Zu et al. (2016) and Mayer et al. (2012), found that a leader’s moral identity and moral attentiveness are associated with followers’ perceptions of ethical leadership behavior patterns. According to Mayer et al. (2012), ethical leadership matters when leaders emulate desired ethical behavior, and use rewards and punishment to reinforce ethical behavior. Under such circumstances, employees are less likely to engage in unethical behavior and practices. Steinbauer et al. (2012) explained how ethical leadership relates to followers’ ethical judgments in an organizational context and found that ethical leadership is positively related to followers’ self-leadership focused on ethics. Okam and Akyuz (2011) found that ethical leadership has a significant, positive correlation with both intrinsic and extrinsic job satisfaction.
Based on the social learning theory, these studies concluded that ethical leadership can impact followers’ ethical behaviors. Brown et al. (2005) and Zu et al. (2016) focused on the relationship between leadership moral identity and development and outcome. However, Steinbauer et al. (2012) supported the deliberate application of self-leadership, with a focus on ethics which leads to higher moral judgment. When Okam and Akyuz (2011) examined the impact of ethical leadership behavior on an employee’s intrinsic and extrinsic job satisfaction, they added that ethical leadership is effective in driving supervisor loyalty and increases job satisfaction. Therefore, the proposed research will attempt to examine the relationship of ethical leadership and patient satisfaction.
Drawing from cognitive evaluation theory, Yidong and Xinxin (2012), proposed a multi-level model to explore how ethical leadership influences employees to adopt innovative behavior in the workplace through the mediation of intrinsic motivation at both individual and group levels. The research revealed that an individual’s innovative workplace behavior was positively related to both individual perceptions of ethical leadership and group ethical leadership, while individual intrinsic motivation mediated the relationship. In addition, the study showed that a group’s intrinsic motivation mediated the relationship between a group’s ethical leadership and innovative work behavior. Some of the study includes the cross-sectional design which prevents the authenticity of causal relationship between the variables. Furthermore, the sample in China may restrict the external validity of the conclusions drawn. The author suggested replicating the study in other cultures and countries.
Ma, Cheng, Ribbens, and Zhou (2013) examined the influence of ethical leadership on employee creativity through the mediation of knowledge sharing and self-efficiency. The participants were employees and supervisors from four Chinese companies. The findings of the research revealed that ethical leadership at the individual level can positively predict employee creativity. Thus, ethical leadership can increase employee creativity through cognitive and motivational mechanisms. Therefore, in order to increase employee creativity, leadership needs to support ethical leadership and encourage behaviors and practices that emphasize knowledge sharing and self-efficiency. The conclusions therein further support the findings of Ta and Lu (2014) which explored the idea that an individual’s innovativeness in the workplace positively related to both individual perception of ethical leadership and group ethical leadership. Therefore, the authors suggested that managers should develop ethical leadership styles by emphasizing morality in the workplace, developing follower’s respect and dignity, and empowering their followers to strive toward innovative practices. These finding stress the vital of ethical leadership on practices which is relevant to the proposed research of ethical leadership and its impact on nursing communication.
Drawing from cognitive evaluation theory, Yidong and Xinxin (2012) revealed that an individual’s innovative workplace behavior was positively related to both individual perceptions of ethical leadership and group ethical leadership, while individual intrinsic motivation mediated the relationship. Ma et al. (2013) revealed that ethical leadership at the individual level can positively predict employee creativity. Yidong and Xinxin (2012) study showed that a group’s intrinsic motivation mediated the relationship between a group’s ethical leadership and innovative work behavior. Moreover, Ma et al. (2013) concluded that ethical leadership can increase employee creativity through cognitive and motivational mechanisms. The conclusions provided further support the findings of Ta and Lu (2012) which explored the idea that an individual’s innovativeness in the workplace positively related to both individual perception of ethical leadership and group ethical leadership
In two multisource studies, Hortog and Belschak (2012) tested a model proposing that work engagement acts as a mediator in the relationship between ethical leadership, employee initiative and counterproductive work behavior. The study investigated whether ethical leadership always forms authentic ethical identity. In a second study, the authors added Machiavellianism to the model which is a strategy of social conduct that involves manipulating others for personal gain. The author did not find support for Brown and Trevino (2006), indicating that Machiavellianism is negatively related to ethical leadership. However, they found that positive effects of ethical leader behavior can be supported when leaders are highly Machiavellian. The first aim of the study was to investigate the role of work engagement in the ethical leadership process. The research finding in both studies revealed that ethical leadership was significantly related to both employee’s initiative and counterproductive work behavior. In addition, these relationships were mediated by work engagement. The findings of these studies suggested that ethical leaders affect followers’ self-esteem and identity by emphasizing the methods by which followers’ effort related to attaining important moral goals and values. This quantitative research was done in the field adding external validity. However, experimental research is stronger when based upon internal validity (Hartoge & Bleschak, 2012). The authors suggested future experimental and longitudinal research to address these limitations.
Yuki, Mahsud, Hassan, and Prussia (2013) assessed the validity of a new questionnaire for measuring aspects of ethical leadership and examined how ethical leadership related to Leadership Member Exchange (LMX) and work performance.
Based on previous theory and research, the author developed and assessed a new ELQ design. The Ethical Leadership Questionnaire (ELQ) is a comprehensive instrument that includes important elements of ethical leadership such as integrity, honesty, fairness, communication of ethical values, ethical behavior, guidance and altruism. The study revealed that the ELQ has high reliability as well as discriminant, criterion – related validity. In addition, the ELQ explained additional variance in both LMX and overall leader effectiveness. The primary purpose on this survey study and analysis was to assess the validity of the new ELQ questionnaire. The findings also revealed that ethical leadership makes a small but significant contribution to the explanation of the leaders’ member exchange and managers’ effectiveness.
Resick, Hargis, Shao and Dust (2013) proposed that ethical leadership is associated with employees’ negative moral equity judgments of workplace deviance, discretionary antisocial behavior such workplace deviance (WPD), and positive moral equity judgments of discretionary prosocial organizational citizenship (OCB). In addition, the authors proposed that these moral equity judgments are cognitive psychological mechanisms that link or mediate the relationship between ethical leadership and employee engagement in both OCS and WPD.
According to Resick (2013), ethical judgments of specific sets of discretionary behaviors link ethical leadership with employee discretionary behavior. The influence of ethical leadership occurs directly among immediate followers, and indirectly across hierarchical level through ethical culture and senior leadership influence (Schaubroeck et al., 2012). Therefore, leaders need to be encouraged in their efforts to embed their assumptions and expectations regarding ethical conduct among organizational followers by creating ethical culture and engaging in ethical leadership practice (Schaubroeck et al., 2012). The ethical work climate can affect the moral contentment of an organization. Ethical leaders can empower their followers to emulate them in participating in ethical decisions that prioritize morality, social value and collective interest within the organization (Choi, Villa, & Kwak, 2015). These findings continue to support the need for further research on ethical climate and organization outcome.
Ethical culture and organization. Organizations are constantly seeking to enhance their members’ creativity, innovativeness, and ethical behavior to gain and sustain a competitive edge in today’s marketplace. Schaubroeck et al. (2012) developed and tested a model linking ethical leadership to unit ethical culture, both across and within organizational levels. The authors examined how both leadership and culture relate to ethical cognition and behaviors of lower level followers.
The research model was drawn from Schein (1985, 2010) to explain senior leaders influence on ethical conduct of followers and subordinates by embedding their expectations and assumptions into the organizational ethical culture. A multilevel model was developed in order to understand how leadership and culture influence ethically-related cognitions and behaviors. The questionnaire of this quantitative research focused only on the effects of higher-level leaders’ behavior and ethical culture outcome at the frontline organizational level. Moral efficiency was measured with five items that was developed by Hannah and Avolio (2010). Ethical culture was measured using the ten-item ethical culture scale (Trevino et al., 1998). Ethical leadership was measured using the 10-items ELS (Brown et al., 2005)
The study revealed that ethical leaders indirectly influence their immediate followers’ cognitions, such as moral efficiency and behaviors, such as transgressions. In addition, ethical leadership influences ethical culture within each hierarchical level, and it extends in parallel level across hierarchical levels. The study found that ethical leadership is positively related to ethical culture of lower levels. Leaders who exhibit high level of ethical leadership may facilitate the influence of subordinate-leader’s ethical leadership on their followers.
Schaubroeck et al. (2012) suggested that leaders should be encouraged to embed their assumptions and expectations regarding ethical conduct throughout the organization. They need to engage in ethical leadership in order to create strong ethical culture. One limitation of this study is the potential to generalize the findings to other organizational context; therefore, the authors suggested further research to be conducted in other type of organizations. The proposed study will focus on nursing ethical leadership impact on healthcare organization.
The organizational leaders’ main task in regards to establishing a culture of character is to lead by example and empower each organizational member to take personal action that demonstrates the organization’s commitment to ethics in its relationship with employees, customers, shareholders, and suppliers (Sims & Suser, 2013). In addition, the leader needs to serve as an ethical role model and mentor to others and must take practical steps to replace maliciousness and indifference with a culture of integrity and honesty, and ethical organization that can secure long term benefits to all (Sims & Suser, 2013).
Demirtas and Akdogan (2015) examined a mediated model of ethical leadership on ethical climate, turnover intention, and affective commitment. The study proposed that managers are role models in their organization when they possess ethical leadership behavior which influences the perception of ethical climate. Ethical leadership was measured using Brown et al. (2005) 10-item ethical leadership scale. The finding of this quantitative correlational study revealed that ethical leadership is significantly correlated to ethical climate, affective commitment, and turnover intention. In addition, ethical leadership behavior is related to the perception of ethical climate, and ethical climate mediates the influence of the managers on individual ethical behavior outcome. The authors emphasized that ethical working environment can benefit both employees and organization. The sample of the study included a wide variety of organizations and job position; however, the sample was not demographically diverse. Therefore, the finding cannot be generalized to other industries or cultures. The authors recommended conducting further research to consider other organizations culture and include additional outcome variables. The proposed research identified the gap, and it will address and examine the relationship of nursing ethical leadership which is a diverse population, and its impact on the variable of nurses’ communication with patients.
Neves and Story (2015) examined the relationship between ethical leadership and organizational deviance through affective commitment to the organization, and proposed this relationship is conditional on the supervisor’s personal reputation for performance; moral standards are coupled with work effectiveness. A sample of 2,024 employees and their respective supervisors was collected from eighteen organizations, including industry, tourisms, service health, counseling, transportation, energy, and financial services. Ethical leadership was measured using Brown et al. (2005) 10-items-scale. This quantitative study used descriptive statistics, reliabilities, and tested the correlation between variables. The finding of the research supported the hypothesis that ethical leadership is significantly related to affective commitment to the organization, especially when supervisors also have a high reputation for performance which in turn is associated with decreased organizational deviance.
The finding suggested that ethical leadership contributes significantly to the development of employee organization relationship (EOR) through social exchange mechanisms. The study found that the strength of the relationship between supervisors’ ethical conduct and employees’ commitment to the organization depends on the supervisor’s reputation for performance. In addition, the researchers found that ethical leadership was indirectly related to employee deviance through an improvement in the EOR. The study found that ethical behaviors combined with high reputations for performance were able to produce the highest level of affective commitment to the organization and the lowest levels organizational deviance. The authors suggested further research to focus on the mechanisms linking ethical leadership and employees’ behavior, particularly how multiple mechanisms operate simultaneously.
According to Sims and Suser (2013), the organizational leaders’ main task in regards to establishing a culture of character is to lead by example and empower each organizational member to take personal action that demonstrates the organization’s commitment to ethics in its relationship with employees, customers, shareholders, and suppliers. Schaubroeck et al. (2012) reveled that ethical leaders indirectly influence their immediate followers’ cognitions, such as moral efficiency and behaviors, such as transgressions.
Sims and Suser (2013) argued the leader needs to serve as an ethical role model and mentor to others and Schaubroeck et al. (2012) suggested that leaders should be encouraged to embed their assumptions and expectations regarding ethical conduct throughout the organization. One limitation of this study is the potential to generalize the findings to other organizational context; therefore, the authors suggested further research to be conducted in other type of organizations. Demirtas and Akdogan (2015) revealed that ethical leadership is significantly correlated to ethical climate, affective commitment, and turnover intention. The authors emphasized that ethical working environment can benefit both employees and organization. Moreover, the authors Demirtas and Akdogan (2015) recommended conducting further research to consider other organizations culture and include additional outcome variables. The finding of Neves and Story (2015) suggested that ethical leadership contributes significantly to the development of employee organization relationship (EOR) through social exchange mechanisms. The study found that the strength of the relationship between supervisors’ ethical conduct and employees’ commitment to the organization depends on the supervisor’s reputation for performance. The main argument of all these studies is that ethical leadership in a key for healthy and productive environment. In addition, in these studies ethical leadership was measured using Brown et al. (2005) 10-items-scale.
Ethical virtues and organizational outcomes. The Greek notion of virtue (arête) means excellence, and it does not separate an individual’s ethics from his or her occupational competence. Both Plato and Aristotle used examples of doctors, coaches, and musicians to point out the relationship between moral and professional excellence. Virtues are dynamic and contribute to an individual’s self-knowledge and self-control (Ciulla, 2012). Virtues provide useful methods of understanding leadership; they encompass moral qualities that an individual can have only if he or she practices them. Virtues, like traits, are dispositions to behave in certain ways. Unlike traits, however, virtues are intentionally selected, deliberately strengthened and behaviorally predictive (Ciulla, 2013).
Kaptein (2008) approaches ethical organizational culture through ethical virtues. Virtue ethics are based on the ideas of Plato and Aristotle and both. Solomon (1999, 2000, 2004 and Kaptein, 1998, 1999) applied the virtue theory in an organizational context. According to the theory, both individuals and organizations require certain virtues for moral behavior. According to Solomon (1992), virtues ethics do not impose prohibit principles or rules of business of behaviors. However, it fosters an intrinsic motivation that leads to successful ethical and business behaviors. Virtue ethics shift the focus from actions and conducts to agent and character (Kaptein, 2016).
Kaptein’s (2011) study had three objectives. The first objective was the collection of data for a broad study of the current status of ethics management in organizations. The second objective was to provide managers with benchmarking information and practical suggestions for managing ethics in their work group. The third objective was to train the analytical and consulting skills of their students. The research findings revealed that six dimensions of ethical culture are negatively related to observe unethical behavior: ethical role modeling management, ethical role modeling of supervisors, capability to behave ethically, commitment to behave ethically, openness to discuss ethical issues, and reinforcement of ethical behaviors. Two of the eight dimensions, clarity of ethical standards and visibility of unethical behavior, were not significantly related to unethical behavior. However, in contrast to previous study of Kish- Gephart et al. (2010), this study found that ethical culture has more powerful effect than ethical climate.
The study of Kish- Gephart et al. (2010), contributed to the understanding and development of theory on organizational ethical culture. It opened several avenues for future research on the relationship between ethical culture and unethical behavior, the internal dynamics of ethical culture, managing and improving organizational ethical culture, and future development of ethical culture measurements. At least six distinct dimensions of ethical culture were relevant in explaining unethical behavior in organizations. In conclusion, this study presented an advanced model for organizational ethical culture assessments.
The study of Kaptein (2011) examined the influence of the ethical culture of organization on employee response to observed wrongdoing. This quantitative study based on 5,065 respondents from the United States consisted of working adults in fifteen selected industries. The author examined the relationship between five types of responses and eight dimensions of ethical culture: clarity, congruency of local management, congruency of senior management, feasibility, supportability, transparency, discussability, sanctionability. The study findings revealed that three internal actions—confrontation, reporting to management and calling an ethics hotline—were positively related to at least four of the eight dimensions of ethical culture. The two other responses—inaction and external whistleblowing—were negatively related to at least four of the eight dimensions of ethical culture.
This study demonstrated that not all the dimensions of ethical culture were related to positive response (internal action) and not all negatively related to negative response (in action and external whistleblowing) from employees who observed wrongdoing. The ethical culture of an organization is important in encouraging employees to correct observed wrongdoing (Kaptein, 2011). The study revealed that four dimensions of clarity, supportability, discussability, and sanctionability are relevant in encouraging employees to intervene and report to management and ethics hotline. The study emphasized the importance of correcting wrongdoing by creating a culture that encourages employees to report and take appropriate action.
Many organizations are adopting ethical programs in order to prevent or reduce unethical behavior. However, the question that faces this organization is which and when to adopt these ethical programs. Kaptein (2015) examined the effectiveness of ethical programs with reference to the scope, composition and sequence of adopted components. This quantitative study was based in 5,065 participants working in different organizations in the US. The unethical behavior was measured by a 36-item unethical behavior scale (Kaptein, 2008). The objective of an ethics program was to influence employee’s behavior promote ethical behavior and inhibit unethical behavior. The impact of ethics programs on employees’ behavior was measured using the CEV model that developed by Kaptein (2008b, 2011b). Nine components of ethics programs were identified and examined.
The study findings revealed that there is a direct relationship between the number of components adopted and the frequency of observed unethical behavior. However, no relationship was found between pre-employment screening and unethical behavior. In addition, the research found that the best sequence for adopting ethics program components is a code of ethics, ethics training and communication, accountability policies monitoring and auditing, and investigating and correction. These five ethical programs were directory related to less unethical behavior. Furthermore, ethics report line, incentive policies, and ethics officers were indirectly related to less unethical behavior.
Riivari and Lamsa (2014) examined the relationship between ethical organizational culture and organization innovativeness. This quantitative empirical study was based on a total of 719 respondents from all levels of Finnish organizations. In this study, the authors applied the corporate ethical Virtues (CEV) model (Kaptein, 2008). This model formulates normative and multidimensional measured of organizational ethical culture evaluations. According to Kaptein (2008), the virtuousness of an organization can be determined but the extent to which the culture of the organization stimulates its members to act ethically and prevent them from acting ethically. The CEV model consists of eight virtues or qualities: clarity, congruency of supervisor, congruency of management, feasibility, supportability, transparency, discussability and sustainability. Organizational innovativeness was measured using Wang and Ahmed (2004) model. The model includes five dimensions: product innovativeness, market innovativeness, process innovativeness, behavior innovativeness and strategic innovativeness.
The study findings revealed that organization’s ethical culture is positively associated with their organizational innovativeness. Different dimensions of ethical culture were found to be inversely associated with different dimensions of organizational innovativeness. The findings of this study suggested that the relationship between ethical culture and organizational innovativeness can be varying between organizations. The researchers found that congruence of management had the highest effect on organizational innovativeness overall and specifically on process and behavioral innovativeness. This research revealed that there is a relationship between ethical organizational culture and specific organizational outcomes and organizational innovativeness. Ethical behaviors of senior management have an important role and effect on organizational innovativeness. The authors suggested conducting further research on ethical leadership related to other group of outcomes such as productivity, efficiency, work satisfaction, and employee commitment.
Huhtala, Feldt, Hyvonen and Mauno (2012) investigated the relationship between ethical organizational culture and a number of personal managerial goals. The purpose of this study was to enrich the knowledge about ethical organizational culture and the manner in which ethical virtues may promote different work goals. This empirical mixed method study was based on a sample of 811 Finnish managers from different organizations in both middle and upper management level. Using quantitative approach, ethical organizational culture was measured using the system CEV questionnaire (Kaptein, 2008). The scale included eight dimensions: clarity, congruency of supervisors and management, feasibility, supportability, transparency, discuss ability, sanction ability.
The research findings revealed that the more ethical the organizational culture was perceived as being, the more organizational goals were reported by managers which relate to organizational success and performance. Ethical organizational culture was a favorable working environment that promotes organizational commitment. The individual CEV dimensions revealed that ethical behavior of supervisors and senior management in particular, alongside supportability and discussability, characterized a favorable working environment that promotes organizational goals. The most important contribution of this study was to establish that ethical organizational culture functions as context for setting personal work goals. Leadership and management practice are important elements related to setting personal work goals. Therefore, organizations need to ensure that their leadership exhibits good examples in ethical actions, reliability, and responsibility.
The study of Huhtala, Mauno and Feldt (2015) aimed to investigate the degree to which employees’ perception of their organizational ethical culture is shared with work units. In addition, this study examined the association between ethical culture and occupational well-being, such as burnout and work engagement, at both individual and work-unit levels. Ethical organizational culture was measured using the 58-item CEV questionnaire (Kaptein, 2008) that included all eight dimensions of the scale. The findings of Huhtala, Mauno and Feldt (2015) study revealed that ethical culture is associated with occupational well-being at both the individual and work unit level. In addition, shared perceptions of ethical organizational culture among work unit members was related to lower burnout and higher work engagement as both outcomes are shared experience. The results of this study are important implications for working life. The CEV scale (Kaptein, 2008) can be used as a practical tool to assess ethical organizational culture in different work units (Huhtala, Tolvanen, Mauno, & Feldt, 2015).
According to Cecilia (1998) and Brown et al. (2005) leadership should be a key source of ethical guidance for an organization. Kaptein (2015) study showed that the effectiveness of an ethics program depends on its scope and composition and the sequence in which the components are adapted. Future research was suggested to include different types of organizations. A study conducted by Huhtala, Kangas, Lamsa and Feldt (2013) aimed to discover whether managers’ self-evaluations of their ethical leadership style was associated with their assessment of the ethical organizational culture. Riivari and Lamsa (2014) study findings revealed that organization’s ethical culture is positively associated with their organizational innovativeness. Different dimensions of ethical culture were found to be inversely associated with different dimensions of organizational innovativeness. Huhtala et al. (2012) found that ethical organizational culture was a favorable working environment that promotes organizational commitment. Huhtala et al. (2015) found that ethical culture is associated with occupational well-being at both the individual and work unit level. The CEV scale (Kaptein, 2008) was used for all these studies and recommended to be used as a practical tool to assess ethical organizational culture in different work units. Therefore, the proposed study will be based on the CEV model Kaptein (2008) and it will address the gap of Riivari and Lamsa’ (2014) study.
Ethical leadership in healthcare. According to Piper (2011) ethics are central to decisions for improving patient care and overall healthcare quality and safety. Ethics come from the moral courage to act for the well-being of others. The organizational mission is central to the delivery of patient care. Therefore, organizational leadership must be accountable to the board and the community in delivering safe and quality care that meets patient expectations.
Healthcare leaders face current and continuous ethical challenges in creating a culture to improve patient safety and quality, while simultaneously reducing medical errors and preventing patient harm and death. Patient and family-centered care is important as it emphasizes patient involvement in their own treatment and inclusion of their families. Hence, patient families are engaged as partners regarding patient decision and intervention.
Healthcare organizations that have succeeded in fostering patient-centered care have gone beyond ordinary contexts of quality improvement, measurement and audit by adopting a strategic organizational approach to patient focus (Luxford, Safran, & Delbanco, 2011). Thus, patient satisfaction is related to the level that patients and families are involved in hospital care. Therefore, in order to improve quality of care and patient satisfaction, patients and their families need to be to be involved throughout the medical care. Patient satisfaction is measured by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS). The survey measures patient experience regarding physicians and nurses’ communication and interactions with patients, responsiveness of hospital staff, pain management, administration of medication, cleanliness of the hospital and quietness of the hospital at night. The patient is also asked to rate the hospital and their willingness to recommend the facility to others.
Nurses are a vital and central component of the healthcare system. These professionals constitute the largest group within the healthcare system. Nursing leadership plays a central role in promoting staff clinical competencies and quality improvement of patient care. Therefore, leaders’ ethical actions and behavior can impact employees’ performance and patient outcomes (Backhand & Shovit Bath, 2016). Thus, ethical competency forms an important part of a nurse leader’s general competency. Leadership ethical competency enables nursing staff to create and adhere to core ethical standards and motivates frontline nursing staff in the provision of care by nurses to patients (Backhand & Shovit Bath, 2016). According to The Joint Commission’s report (TJC; 2008), intimidating and disruptive behavior can foster medical errors, decrease patient satisfaction, increase costs, and foster outcomes which may cause qualified employees to leave the organization. The majority of clinicians are seeking to work in a healthy and ethical environment. Therefore, zero tolerance for disruptive behavior can improve collaboration and cooperation among healthcare employees.
Gokce, Guney, and Katrinli (2014) aimed to determine the doctor’s perception of leadership behavior and their commitment to the organization. The study focused on the concepts of leadership, organizational commitment, and organizational culture. This study revealed that organizational commitment of doctors is positively related to leadership behavior. However, organizational culture did not act as a moderator in the relationship between leadership and organizational commitment. The research findings suggested that leadership behavior, as perceived by doctors, have an effect on their organizational commitment and less effect on organizational culture. The main limitation of this study was the single location and the limitation to one group of healthcare providers. Therefore, the authors suggested further research to include nurses, administrative staff, and other diverse groups of healthcare employees. The proposed study will focus on frontline nursing staff perception of ethical leadership.
According to the National Center of Ethics in Healthcare (NCEHC) in the Department of Veterans Affairs (VA), ethics quality means that healthcare organizational practices must be consistent with widely accepted ethical standards, norms, and expectations of the healthcare organization (Foglia et al., 2012). In order to improve ethics quality in healthcare, organizations need to examine their overall ethical practices, consistency and alignment with the organization’s standards, norms, and expectations (Pearlman, Bottrell, Altemose, Foglia, & Fox, 2013).
Foglia, Cohen, Pearlman, Bottrell, and Fox (2013) evaluated the association between employee sensitivities to ethical leadership (EL), ethical environment culture (EEC) and perceptions of the organization’s overall ethical quality. The study analyzed 88,605 VA employees’ responses to the 2010 IESS questions. The purpose of this study was to characterize employee perceptions of EL/EEC in VA hospitals, and to evaluate the association between employees’ perceptions of EL/EEC and perceptions of the organization overall ethics quality. The research revealed that physicians and employees with higher levels of supervisory responsibility were more likely to have positive perceptions of EL and EEC concepts as related to overall organizational ethics quality. Most VA employees perceived their organization as ethical when employees are treated fairly. VA manager and physician perceptions of organizations ethics were more than non- physician and non-managers employees. Different VA facilities perceptions of organizational ethics vary considerably across facilities. The findings of this study support the important relationship among ethical leadership, organizational environment and culture, and connections to ethics quality (Foglia et al., 2013).
According to Fox (2012), in order to evaluate ethics quality, a well-defined conceptual model is imperative, along with an expert team of evaluators, commitment to responsiveness, availability, and tailoring the evaluation methods to the target audience. One of the innovative aspects of integrated ethics is that it emphasizes that ethical practices in healthcare organizations depend not only on specific decisions and actions, but also on the organizational system and processes that influence decision-making and implementation (Crigger & Wynia, 2013).
The moral dimensions of the ethical leader refer to their strategies to influence their followers’ ethical conduct. These strategies can be affected through role modeling of ethical behavior, setting clear ethical standards, and the implementation of reward and punishment to ensure compliance with established standards. Chughtai (2015) examined the effect of ethical leadership on safety, performance, and the mediating role of job autonomy and self-efficiency on this relationship. The findings of the research revealed a positive relationship between ethical leadership and both self-efficiency and job autonomy. Ethical leadership behavior can have an impact on the components of performance, safety compliance and safety participation.
Walumbwa, Morrison, and Christensen (2012) suggested that ethical leadership can lead to higher in-role performance for groups of staff. The authors argued that the two key mechanisms of the group are: group conscientiousness, which is the emergent state, and group voice which is the group process. The study revealed a strong positive relationship between ethical leadership and group in- role performance. The study suggested that, when leaders were perceived by their members as ethical and displayed high levels of ethical behavior, the group members performed more effectively. Hence, ethical leadership is an important factor of group in-role performance which can lead to better organizational outcomes. In addition, the group consciousness and group voice mediated the ethical leadership-group performance relationship. The conclusion highlights the practical value of group voice for group performance. In addition to the theoretical implication, the study may have practical implications in creating high performance teams which demonstrate high ethical standards, model ethical conduct, and benefit in the rewards associated with ethical compliance and activities.
The study of Suhonen, Stolt, Gustafsson, Katajisto, and Charalambous (2014) revealed association between ethical climate, the professional practice environment and the level of perceived individualized care. The study emphasized that ethical climate is an important determinant of individualized care. Utriainen, Ala-Mursula, and Kyngas (2015) performed a study aimed at developing theoretical models of hospital nurses’ well-being within the workplace. According to the theoretical model, the well-being of hospital nurses at work is constructed upon patients experiencing a high quality of care, support among nurses, cooperation, collaboration, satisfaction, challenging and meaningful work, freedom of expression, opportunity for professional development, two-way communication, and fair and supportive leadership. The study revealed that collegial relationships, meaningful professional development and fair leadership play a major role in well-being of hospital nurses. Agheorghiesei, Iliescu, Gavrilovici, and Opreas’ (2014) study aimed to identify hospital executive opinions regarding the relevance of ethical audit procedures in the accreditation process of Romanian hospitals. The study revealed that Romanian managers consider the introduction of ethical audit within the accreditation process as relevant and appropriate. They believe that ethical monitoring is beneficial for healthcare organizational performance. Ethical auditing could impose standards and requirements in the healthcare system which are productive and improve ethical performance in healthcare.
Walumbwa et al.(2012) revealed that ethical leadership is an important factor of group in-role performance which can lead to better organizational outcomes The study of Suhonen et al. (2014) also revealed association between ethical climate, the professional practice environment and the level of perceived individualized care. In addition, Chughtai (2015) suggested that ethical leadership behavior can have an impact on the components of performance, safety compliance and safety participation. The findings of Foglia et al. (2013) study support the important relationship among ethical leadership, organizational environment and culture, and connections to ethics quality. However, according to Utriainen et al. (2015), collegial relationships, meaningful professional development and fair leadership play a major role in well-being of hospital nurses. Agheorghiesei et al. (2014), added that ethical monitoring is beneficial for healthcare organizational performance. Gokce et al. (2014) examined doctors’ perception of leadership behavior and their commitment to the organization and suggested further research to include other healthcare professional such nurses. Nurses are a essential and crucial component of the healthcare system. The proposed research will focus on nurses’ perception of organizational ethical culture and its impact on patient satisfaction related to nurses’ communication.
According to Wong (2015), the mechanism of leadership effects on patient outcome is a very challenging topic and to date many of its impact is unknown. However, there is a connection between supportive leadership approach and positive patient safety outcome which includes lower medication errors, nosocomial infections and patient satisfaction (Wong, Cuming, & Ducharme, 2013). Healthcare leaders have considerable influence in the healthcare delivery due to their role and responsibilities. Walumbwa et al. (2012) suggested that ethical leadership can lead to higher in-role performance for groups of staff. Ethical leadership can improve workplace safety (Chughtai ,2015). Therefore, organizations need to develop and select ethical leaders. Collegial relationships, meaningful professional development and fair leadership play a major role in well-being of hospital nurses (Suhonen et al., 2014). Agheorghiesei et al. (2014) added that ethical monitoring is beneficial for healthcare organizational performance. Therefore, healthcare leaders require a shared vision approach that engagement of all their members in order to achieve this powerful and more lasting vision (Cumming, 2012). Ethical practices, values and principles are the foundation of the moral action and decision-making of professional practices. Nurses have an obligation to provide quality patient care. Therefore, nursing leadership has a major role in creating moral and ethical environments that are based in ethical practices (Bejarnason & Lasala, 2011). Patient satisfaction is part of patient evaluation of their care. Patient feedback provides an opportunity for healthcare organizations to establish strategic planning for healthcare quality improvement
Patient satisfaction. Healthcare systems continue to face challenges including high costs of technology, diminishing resources and an increasing demand for high quality and safe care. Financial sustainability is a key to survival. One important factor of sustainability in healthcare is the social component. The social component focuses on the organization’s identity and culture which includes collaboration, coordination, empowerment, diversity, equity, justice and fairness for all. Patient satisfaction is a key factor of the social element. Hence, this element is representative of the patient‘s experience regarding, service, accessibility, cost, quality and safe care.
The Center for Medicare and Medicaid Services (CMS, 2013), for the implementation of Value-based purchasing, tied hospital reimbursement to quality-care metrics, including patient ratings of their care experience, with a special emphasis on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) rating. These reimbursement standards placed further emphasis on the quality of care in general and patient perceptions of their care experiences, specifically.
The CMS designed financial metrics which reward or penalize hospitals according to their HCAHPS scores. Such measures of patient satisfaction coupled with perceptions regarding their care can be significant in guiding healthcare organizations in terms of their operations and practice decisions. This low-cost methodology can yield out-sized returns through the adoption of best practices and responsiveness to patient needs and concerns. This management tool can assist organizations in improving patient outcome, organizational sustainability and stability. Hence, these metrics may enable healthcare organizations to retain current patients, attract new ones, and streamline the work flow throughout the organization.
The goal of patient satisfaction surveys is to understand (from a patient’s perspective) the quality of care, specific strengths and weaknesses, and identify areas where the delivery of care may be improved. The interest of measuring patient satisfaction was initiated and developed through the Center for Medicare and Medicaid Services (CMS), and The Agency of Healthcare Research and Quality (AHRQ). These initiatives resulted in the development of The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS). Patient satisfaction surveys also address the humanism of healthcare professionals. This survey touches upon qualities such as caring, compassion and concern, and the responsiveness of the healthcare professional to patient needs and concerns. The second important element of humanism and respect is two-way communication skills. This component is critical to patient care, planning, intervention and decision-making. Therefore, central patient care places patients and their families at the center of effective communication between professional and patient outcome. In addition, patient satisfaction surveys address patient safety and confidentiality.
Patient satisfaction surveys offer and assess whether health professionals communicate and explain important information, as well as, the side effects of medications which are being administered. Patient understanding of their medications and side effects can provide guidance when seeking medical attention. However, patient satisfaction surveys do not address other hospitals associated problems such as infections, surgical complications, readmission rates and death rates (Junewicz & Youngner, 2015). The relationship between patient satisfaction and quality of care is still, largely unclear (Junewicz & Youngner, 2015). Quality of patient care can encompass many different aspects of healthcare, and to date no clear evidence exists to demonstrate that patient satisfaction data improves healthcare quality and safety. In addition, patient satisfaction scores can be biased due to patient’s mental status, patient’s desire and demands for drugs, and it can pressure providers to administer inappropriate care (Junewicz & Youngner, 2015).
The extent of nursing influence on patient satisfaction may be manifested by the HCAHPS survey. Parameters related to nursing interactions are included throughout the survey questionnaire. Measurements of nursing responses to patient needs include variables such as responding to call bells, treating patients with courtesy and respect, room quietness at night, communication of the nurse regarding patient care, medication requirements and discharge planning. Therefore, patient perceptions of the frontline nursing staff are a key element in patient satisfaction scores. In the clinical setting, nurses often value clinical leaders who embrace and operate with a strong moral compass (Mannix, Wilkes, & Daly, 2015). Therefore, a leadership style that incorporates an esthetic world view with a strong moral purpose can enhance the clinical nursing workplace.
Bjerdnaes et al. (2012) study investigated the effects of different predictors of overall patient satisfaction with hospital experience. Patient experience questions were based on the patient experiences questionnaire which comprised of 26 items including two items about expectations, one item about overall patient satisfaction, 14 questions about quality of life and 10 background questions. The research finding revealed that thirteen variables were significantly associated with overall patient satisfaction; two variables about fulfillment of expectations, eight about patient reported experience and three sociodemographic variables. The most important predictor of patient satisfaction with hospitals was patient reported experience with nursing service, followed by fulfillment of patient expectations, experience with doctors’ services, and perceived appropriate treatment.
Szecsenyi et al. (2011) research aimed to evaluate whether there is an association between patient satisfaction and job satisfaction of healthcare teams. The research revealed a positive correlation between non-physicians’ team members (nurses and others) and patient satisfaction. High job satisfaction by non-physicians was associated with high patient satisfaction. The result of this study revealed that satisfaction of non-physicians has a larger impact on patients’ evaluation on quality of care than the satisfaction of the physicians. One limitation of this study is limited sample and location.
Boev (2011) study first aim was to examine patient perception of nursing care associated with their hospitalization in the intensive care unit (ICU) using their existing unit of patient satisfaction survey. The second aim was to describe nurses’ perception of work environment with a defined sample of adult critical care units, using the Practical Environment Scale of the Nursing Work Index (PES-NWI). The last aim was to explore the relationship between nurses’ perception of work environment and patient satisfaction in the ICU using multilevel modeling as the basis for statistical analysis.
The research finding revealed that patients were very satisfied with their hospitalization. Nurses reported moderate satisfaction with work environment. Perception of nurse manager leadership and ability was significantly related to patient satisfaction. Favorable perception of the nurse managers was associated with increased patient satisfaction. The research provided preliminary support for the relationship between nurses’ perception of work environment and patient satisfaction in adult critical care. However, some limitation present due to secondary data, sample size, and the patient satisfaction instrument that has not been tested fully. Therefore, the researcher suggested further studies exploring the relationship between nurse perception and patient outcome.
Ancarani, Di Mauro, & Giammanco, 2011) tested a model of organizational climate, its perception by medical and nursing staff and the impact on patient satisfaction. This cross-sectional study was based on a sample of 2,563 which consisted of 57 managers, 848 employees (621 nurses and 277 physicians), and 1,598 patients. The research found that different climates impact patient satisfaction differently, and human relation climate increases patient satisfaction. There is evidence in favor of the mediating effect of climate between the managers’ climate orientation and patient satisfaction. The researchers suggested that in order to improve patient satisfaction in hospital units, managers should improve climate toward staff coordination, cohesion, support and staff welfare. The main limitation of this study is the cross-sectional nature of the data. The researchers suggest further research in different setting of healthcare.
Aiken’s (2012) research aimed to investigate whether healthcare organization with improved nurse staffing and work environment can affect patient care and nurse work stability, in European countries. This research also was based on a cross-sectional study of 1,105 general acute hospitals, 488 in European countries, and 617 in four states in the United State. Patient satisfaction was measured using the Hospital Consumer Assessment of Healthcare Providers and System, (HCAHPS) instrument. The research findings revealed that patients in hospitals with better work environment were more likely to rate their hospital highly and recommend their hospitals. The study in these different countries indirectly indicates that organizational behavior and the retention of a qualified and committed nurse work force might be a promising area to improve hospital care safety and quality both nationally and internationally. One of the limitations in the study was that it relied on cross-sectional data which could not definitively establish causality.
Effective leadership in healthcare is important for the achievement of optimal patient outcome. Wong, Cummings, and Ducharme (2013) in their systematic review of studies, examined the relationship between nursing leadership practices and patient outcome. A total of 20 studies suggested positive relationships between leadership styles and higher patient satisfaction, lower patient mortality, fewer medication errors, less restraint use and fewer hospital-acquired infections. The findings of this study provided support for the assertion that relational leadership practices are positively associated with the same categories of patient outcome. Effective leadership approach contributes to a healthy work environment which is through continual support, open and honest communications and trust (Wong et al., 2013). Trustworthy managers can inspire nurses’ commandment to their willingness to be engaged in patient care quality decisions. The dialogue and communication between leadership and frontline nursing staff to resolve patient care issues can decrease patient dissatisfaction, increase patient safety and quality care outcome (Wong et al., 2013).
Nursing provides a holistic approach to patient care; hence, the relationship between the nurse and patient is therapeutic and based on trust and mutual understanding, as well as open communication which fosters mutual goal setting (Peplau, 1997). The implication of effective communication to the patient can lead to increased patient satisfaction, prevent loss of reimbursement, and potentially increase referrals. Improved nurse-patient communication would improve quality care, support a decrease in anxiety, elevate safety, and enable patients to develop trust in nursing care, which potentially may lead to improved patient outcomes. In essence, improved staff communication skills would eventually increase patient satisfaction (Oni, 2012). Based on the history of patient satisfaction, a great need exits to understand how healthcare leaders can sustain consistently high patient satisfaction scores within a department/unit. This research study will raise awareness within the healthcare sector as to how nursing leadership ethics can influence and sustain HCAHPS scores in the 90th percentile.
A Press Ganey’s (2013) study identified Communication with Nurses as a rising tide measure among the eight HCAHPS dimensions of care. A rising tide measure is one whose change and trajectory in performance is correlated with multiple measures. This effect is important to understand when devising performance improvement strategies, for as the score of a rising tide measure increases, the scores of the associated measures are likely to rise as well.
Using data from a robust sample of 3,062 United States acute-care hospitals in the CMS Hospital Compare Database, Press Ganey’s (2013) research team conducted a hierarchical variable clustering analysis on all eight HCAHPS dimensions. The data was collected between October 1, 2009, and September 30, 2010, and was analyzed by performing a hierarchical variable clustering analysis on all eight HCAHPS dimensions. This type of analysis is different from a traditional correlation analysis, which looks at the relationship between two measures only. The variable clustering technique identifies multiple measures that “hang together” consistently, and the hierarchical analysis identifies which measure (or cluster of measures) leads the others. The objective of the analysis was to find out the leader of the HCAHPS dimensions and assist hospitals to strategically focus their performance improvement resources on high impact issues.
Press Ganey’s (2013) analysis identified five HCAHPS dimensions that consistently cluster together: communication with nurses, responsiveness of hospital staff, pain management, communication about medication, and overall rating. The finding revealed that communication with nurses led the other four measures. This means that when a hospital aims improvement efforts on the communication with nurses’ dimension, it can lead to gains in performance in the other four dimensions in the cluster.
The CMS designed financial metrics which reward or penalize hospitals according to their HCAHPS scores. Effective leadership in healthcare is important for the achievement of optimal patient outcome. Effective leadership approach contributes to a healthy work environment which is through continual support, open and honest communications and trust (Wong et al., 2013). Nursing provides a holistic approach to patient care. Patient satisfaction surveys offer and assess whether health professionals communicate and explain important information. The implication of effective communication to the patient can lead to increased patient satisfaction and prevent loss of reimbursement. Oni (2012) argued that improve staff communication can lead to improve patient outcome. A Press Ganey’s (2013) study identified Communication with Nurses as a rising tide measure among the eight HCAHPS dimensions of care. Press Ganey’s (2013) analysis revealed that that communication with nurses led the other four measures such as responsiveness of hospital staff, pain management, communication about medication, and overall rating. However, According to Junewicz and Youngner (2015) quality of patient care can encompass many different aspects of healthcare, and there is no clear evidence exists to demonstrate that patient satisfaction data improves healthcare quality and safety.
According to Szecsenyi et al. (2011) the most important predictor of patient satisfaction with hospitals is patient reported experience with nursing service, followed by fulfillment of patient expectations, experience with doctors’ services, and perceived appropriate treatment. In addition, the study of Boev (2011) added that Perception of nurse manager leadership and ability was significantly related to patient satisfaction. Ancarani et al. (2011) suggested that in order to improve patient satisfaction in hospital units, managers should improve climate toward staff coordination, cohesion, support and staff welfare. The researchers suggested further research in different setting of healthcare. The proposed study will focus on nursing ethical leadership impact on nurses’ communication.
Methodology. As evidence by the preceding review of literature, many quantitative studies and very few qualitative studies have been conducted. The literature review proceeded with ethical leadership perception. Jordan et al. (2013) quantitative study proposed that followers’ perception of ethical leadership depends on the executive leader’s cognitive moral development (CMD). The authors explain his findings by using the social learning theory framework. The study was cross sectional with limited samples of senior executives. However, the social learning theory supported the study direction. Drawing for the social learning theory, Steinbauer et al. (2012) tested and developed two stage models in order to investigate ethical leadership correlation to followers’ ethical judgment an organizational content. This quantitative correlational study used single item measures for perceived accountability and achieves judgment due to time and space limitations. In addition, the author defended their use of vignettes by pre-testing several vignettes with manipulation check to validate their conditions and they selected the best-improved vignette that fit the research design.
The two studies of Mayer et al. (2012) were drawn from the social learning and moral identity theories examined antecedents and consequences of ethical leadership. This quantitative correlational study tested their theoretical model using data collected in two large scale unit-level field studies, using parsimonious structural equation models with data collected from a variety of sources, organizations, and industries. Ethical leadership was compared to related leadership construct through confirmatory factor analyses (CFA). The authors examined models that included idealized influence, interpersonal justice, and informational justice as the primary mediation. Each model was examined with and without the other leadership variables serving as controls. This research explained the effects of ethical leadership in units from a variety of industries and organization. The study of Resick et al. (2013) used samples through Study Response service that using complete online survey (Stanton & Weiss, 2002). This quantitative cross-sectional study applied a social cognitive lens in order to understand the relationship between ethical leadership and ethical cognition and discretionary behaviors. This study was based exclusively on the individual level of analysis.
Schaubroeck et al. (2012) study also indicated that ethical leadership across multiple levels is related to unit level culture and behaviors. In the quantitative methodology of Demirtas and Akdogan (2010), several precautions were taken to minimize common methods biases by designing the data collection procedure where the independent and dependent variables collection performed in different times. Moreover, the survey was conducted face to face to reduce the mistakes of questionnaires and variables. The study of Neives and Story (2015) also was grounded on the social exchange theory. This quantitative study used descriptive statistics, reliabilities and tested the correlation between variables.
Kaptein (2008) approaches ethical organizational culture through ethical virtues. A quantitative empirical research conducted. An exploratory factor analysis provided support in the existence of eight unidimensional corporate ethical virtues: clarity, congruency of supervisor, congruency of management, feasibility, supportability, transparency, discussability, and sanctionability (Kaptein, 2008). The research on organizational ethical culture is growing. However, there is still need for more theoretical knowledge and empirical findings (Huhtala et al., 2013). In order to improve ethical quality in healthcare organizations, there is a need to examine their overall ethical practices, standard and expectation, alignment and consistency with norms (Pearlman et al., 2013). Quantitative research methodology was appropriate for the study for its preciseness in measuring the variable (dependent, independent, and control variables).
There is no single blueprint for planning research. Research design is governed by the notion of fitness for purpose. The purpose of the research determines the methodology and design of the research (Cohen, Manion, & Morrison, 2011).The quantitative correlational design is the most effective methods to investigate the relationship between two variables, it is provide numerical estimates of the relationship with a comparison of the strength of any identified differences between the two variables (Cohen et al., 2011).Correlation techniques are generally intended to answer three questions about two variables or two sets of data. First “Is there a relationship between the two variables or set of data? When the answer is “yes” two other questions will follow “what is the direction of the relationship?” and “what is the magnitude?” (Cohen, 2000). Quantitative research methods provide strategies to conduct systematic and controlled statistical test to measure and conform hypotheses (Hogan, 2014). Therefore, a quantitative methodology will be conducted to investigate the relationship between nursing ethical leadership virtues and organizational outcome of patient satisfaction.
Instrumentation. The majority of literature review studies on ethical leadership used Brown et al.’s (2005) ten-items ethical leadership scale (Stanbaure et al., 2012; Mayer et al., 2012; Okam & Akyuz, 2011; Yidong & Xinxin, 2012; Ma et al., 2013; Hortog & Belschak, 2012; Resick et al., 2013; Demirtas & Akdogan, 2013; Neves & Story, 2015). Brown et al (2005) developed the Ethical Leadership Scale (ELS) to measure perception of ethical leadership. Initial, it included 48 items of ethical leadership using the results from previous qualitative studies by Trevino et al. (2000; 2003). The final result of Brown et al. (2005) study was 10-items: Listens to what employees have to say”. “Disciplines employees who violates ethical standards” “Conducts his/her personal life in an ethical manner.” Has the best interests of employees in mind. ”Makes fair and balanced decisions”. “Can be trusted”. “Discusses business ethics or values with employees.” “It is an example of how to do things the right way in terms of ethics.” “Defines access not just by results but also the way that they are obtained.” and “when making decisions, ask “what is the right thing to do?”. Brown et al. (2005) scale has been tested and validated extensively, and its consists of small set of items However, some researchers criticize the ELS due to lacking of relevant aspects of ethical leadership such honest communication, behavior consists with exposed values, and for allocation is assignments and records (Yuki et al., 2013).
The ten-item Ethical Leadership Scale (ELS), which was developed by Brown et al. (2005) was used by many studies to examine the impact of ethical leadership in organizational outcome; the correlation between ethical leadership and leadership’s influence on five major dimensions of behavior (Xiaoyong et al., 2011); the effect of ethical leadership on safety, performance, and the mediating role of job autonomy and self-efficiency on this relationship (Chughtai ,2015); the relationship between ethical leadership and group in- role performance (Walumbwa et al., 2012). However, Gokce et al. (2014) used the Multifactor Leadership Questionnaire (MLQ) developed by Avolio and Bass (1995) to identify the doctors” perception of leadership behaviors. In addition, Foglia et al. (2013) evaluated the association between employee sensitivities to ethical leadership (EL), ethical environment culture (EEC) and perceptions of the organization’s overall ethical quality. The authors examined employee perception of ethical practices utilizing the Ethical Leadership Compass (ELC). The ELC is a tool that brings insights and principles of organizational and business ethics together in order to encourage leaders to create an environment which fosters ethical behavior throughout their daily routines.
Kaptein (2008) approaches ethical organizational culture through ethical virtues. The CEV model takes normative stands towards ethical culture by strengthening the eight keys. The CEV scale consists of 58 items, which are classified to eight factors of organizational virtues: clarity which refers to expectations concerning ethical conduct of employees, it is consists of ten- items such “The organization makes it sufficiently clear to me how I should conduct myself appropriately towards others within the organization. The second and third virtues refer to congruency; congruency of supervisor, and congruency of management. There are two virtues emphasize the importance of managers and supervisors in the organization and the example that they set. It consists of a total of 10 items such “My supervisors set a good example in terms of ethical behavior”. The fourth virtue, feasibility, concerns the conditions and availability of resources in the organization in order to meet expectations. It consists six items such “In my immediate working environment, I am sometimes asked to do things that conflict my increase.” The fifth virtue, supportability, it refers to how the organization helps and support employees to meet normative expectations of ethical behavior. It consists six items such “In my immediate working environment, and atmosphere of natural trust prevails “The six virtues is transparency, it refers to the degree to which the consequences of the conduct are visible to everyone in the organization. It is consisted of seven items such “If a colleague does something that is not permitted, my manager will find out about it”. The seven virtues, discussability refers to employees’ opportunities to discuss ethical issue. It consists of ten items such “In my immediate environment, reports of unethical conduct are handles with caution.” The eight and the last virtue is sustainability which refers to the likelihood of employee’s reward of ethical behavior and punishment for unethical behavior. It is consisted of nine items such “In my working environment, people are accounted of their actions”.
Kaptein (2016) argued that ethical leadership can also be viewed as leadership in ethics, apart from being a moral person and moral manager, and ethical leader is a morality innovator who establishes a new ethical norm that followed successfully. Moreover, the characteristics of leadership in ethics are that it is transitional, multilevel and issue specific which can open new avenue, of studying antecedents and outcome of her ethical leadership. In the literature review, the CEV model applied to some studies (Kaptein, 2008, 2009, 2010, 2011, 2015; Solomon & Hanson, 1985; Solomon, 1992, 2004; Riivari et al., 2012; Huhtala et al., 2013; Huhtala et al., 2011; Huhtala, 2013; Huhtala et al., 2015; Kangas et al., 2014).
According to Cohen et al. (2015), when healthcare organization possess high level of ethical culture, they experience less staff turnovers, more productivity, better level of patient safety, cost saving and high level of patient satisfaction. Therefore, improving employee’s perceptions of ethics in the organization could have impact on healthcare organizational outcome. The ethical culture of the organization will be measure with the CEV questionnaire (Kaptein, 2008) the structure of the CEV scale for measuring and evaluation ethical culture has been previously tested and validated by researchers (Kaptein, 2008; Huhtala et al., 2011; Riivari et al., 2012). The background variables (Gender, age, education and position) had significant correlations with some of the CEV dimensions. Therefore, the study will also use these variables and nursing years of service.
Patient satisfaction will be measured using the Opinion Meter which is based on the existing HCAHPS survey. The version of the inpatient HCAHPS survey is comprised of 32 core items. The survey includes twenty-one questions and encompasses nine key topics: communication with nurses, communication with doctors, responsiveness of hospital staff, pain management, communication about medicine, discharge information, cleanliness of the hospital environment, quietness of the hospital environment, and transition of care (CMS, 2013).
Patients after discharge will be asked to answer the survey questions about their stay at the hospital, the HCAHPS survey includes 32 questions (Appendix G), and it will be mailed to discharge patients form inpatient units. There are four questions regarding nurses’ care during this hospital stay: how often did nurses treat you with courtesy and respect? how often did nurses listen carefully to you? , how often did nurses explain things in a way you could understand? , and after you pressed the call button, how often did you get help as soon as you wanted it? . The predictive validity of a patient satisfaction instrument (HCAHPS) shows high levels of predictive validity. Additionally, multiple regression analyses revealed that, collectively, all items are significant predictors of patient’s reported experiences (Press Ganey, 2013). HCAHPS’ reliability ranged from .78 to .95. The Cronbach’s alpha for the entire questionnaire is .97, confirming the instrument’s high internal consistency and reliability. The inpatient instrument was found to be psychometrically sound across a wide variety of tests of validity and reliability (Press Ganey, 2013).
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| REVIEW OF THE LITERATURE This section provides a broad, balanced overview and synthesis of the existing literature related to the proposed research topic. It identifies topics, themes, trends, and conflicts in research methodology, design, and findings. It describes the literature in related topic areas and its relevance to the research topic and research approach. It provides an overall analysis and synthesis of the existing literature examining the contributions of this literature to the field; identifying the conflicts; and relating the topics, themes, and results to the study topic and research approach. Accurate, empirical research citations are provided for all ideas, concepts, and perspectives. The researcher’s personal opinions or perspectives are not included. (Minimum 30 pages) | ||||
| This section must be a minimum of 30 pages. The purpose of the minimum number of pages is to ensure that the overall literature review reflects a foundational understanding of the theory or theories, literature and research studies related to the topic. A well-written comprehensive literature review that reflects the current state of research and literature on the topic is expected and will likely exceed 30 pages. Literature review should be updated continuously. This is an ongoing process to dissertation completion. | 2 | 2 | X | |
| Quantitative Studies: Describes each research variable in the study discussing the prior empirical research that has been done on the variables and the relationship between the variables. Qualitative Studies: Describes the phenomena being explored in the study discussing the prior research that has been done on the phenomena. | 2 | X | ||
| Themes or Topics (Required): Discusses and synthesizes studies related to the proposed dissertation topic. May include (1) studies describing and/or relating the variables (quantitative) or exploring related phenomena (qualitative), (2) studies on related research such as factors associated with the themes, (3) studies on the instruments used to collect data, (4) studies on the broad population for the study, and/or (5) studies similar to the proposed study. The themes presented and research studies discussed and synthesized in the Review of Literature demonstrates a deep understanding of all aspects of the research topic. | 2 | 2 | X | |
| Methodology Section (required): Discusses and synthesizes the various methodologies and designs that have been used in prior empirical research related to the study. Must use authoritative sources to justify the proposed design. | 2 | 2 | X | |
| Instrumentation Section (required): Provides discussion and justification for the instrumentation selected for the study. This section must argue the appropriateness of the dissertation’s instruments, measures, and/or approaches used to collect data. Empirical research must be used to justify the selection of instrument(s). | 2 | 2 | X | |
| Structures literature review in a logical order, includes actual data and accurate synthesis of results from reviewed studies as related to the learners own topic, not just a summary of the findings. | 2 | 2 | X | |
| Includes in each major section (theme or topic) within the Review of Literature an introductory paragraph that explains why the particular theme or topic was explored relative to the overall dissertation topic. | 2 | 2 | X | |
| Includes in each section within the Review of Literature a summary paragraph(s) that (1) compares and contrasts alternative perspectives on the topic and (2) provides a synthesis of the themes relative to the research topic discussed that emerged from the literature, and (3) identifies how themes are relevant to the proposed dissertation topic. | 2 | X | ||
| Provides additional arguments for the need for the study that was defined in the Background to the Problem section. | 2 | 2 | X | |
| Ensures that for every in-text citation a reference entry exists. Conversely, for every reference list entry there is a corresponding in-text citation. Note: The accuracy of citations and quality of sources must be verified by learner, chair and committee members. | 2 | X | ||
| Uses a range of references including founding theorists, peer-reviewed empirical research studies from scholarly journals, and government/foundation research reports. Note: A minimum of 50 peer-reviewed, empirical research articles are required for the literature review. | 2 | 2 | X | |
| Verifies that 75% of all references are scholarly sources within the past 5 years. The 5 year time frame is referenced at the time of the proposal defense date and at the time of the dissertation defense date. Note: Websites, dictionaries, publications without dates (n.d.), are not considered scholarly sources and should not be cited or present in reference list. | 2 | 2 | X | |
| Avoids overuse of books and dissertations. Books: Maximum of 10 scholarly books that present cutting edge views on a topic, are research based, or are seminal works. Dissertations: Maximum of 5 published dissertations. | 2 | 2 | X | |
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | X | |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Summary
The issue of ethics in business is a global problem. The challenges facing healthcare requires strong leadership. The healthcare industry is unique because it depends upon human beings caring for one another. Thus, patient care is dependent on healthcare professionals. Therefore, the importance of aligning the working environment through collaboration, cooperation, and setting of ethical standards directly empowers leadership and healthcare professionals to provide patients with the highest of quality care. Ethical leadership is important because it decreases the deleterious effects of stressful work environments (Xiaojun & Guy, 2014). Ethical cultures contribute to teamwork, enhance job satisfaction and encourage the accomplishment of the organization’s mission and objective (Lu & Lin, 2014).
Ethical leadership is an important aspect of creating virtuous climates in which both nursing and patient outcome can be enhanced (Markarott, Storch, Pauly, & Newton, 2014). Professionals invoke specific moral assumptions. Healthcare professionals’ morality should be embedded in policies, customer service and practices (Deherty & Purtilo, 2015). When managers apply ethical leadership style through demonstrations of fairness, power sharing, ethical guidance, role clarification and integrity in their behavior and action, employees become more trusting and organizational commitment can increase (Nastiezaie, Bamer, & Salajage, 2016).
In summary, the literature reveals several areas of interest regarding organizational ethical culture. Many studies have shown that ethical leadership directly influences follower attitude and behavior in the work environment (Yidong & Xinxin, 2013; Neubert, Wu, & Roberts, 2013; Schaubroeck et al., 2012; Kacmar, Carlson, & Harris, 2013). Ethical leadership focuses on sustaining and encouraging followers’ ethical conduct (Stouten, Van Dijke, & De Cremer, 2012). Ethical leadership has significant influence on the regulatory mindset of employees and their behavior in the workplace (Neubert, Wu, & Roberts, 2013). The topic of ethical culture plays a critical role in organizational innovativeness and subsequent, sustainable performance (Riivari & Lasma, 2013). When employees perceived their leaders to be ethical, such workers exhibited elevated levels of corporate citizenship, higher performance achievements, and greater job satisfaction (Sharif & Scandura, 2014).
A review of the literature involved the definition of ethics, ethical leadership, ethics within organizations, ethical leadership specifically within healthcare organizations and patient satisfaction. The review of these key organizational functionalities revealed supportive evidence of the importance of ethical leadership in organizational outcomes. The literature revealed that ethical leadership is significant for motivating employees and improving organizational performance. Many aspects of nursing leaders remain unexamined and need to be explored through more studies and need to be performed (Stanley 2008, Patrick, 2011). It is clear that more attention needs to be paid to ethics and values in nursing leadership, particularly the role of integrity (Hutchinson & Jackson, 2013). However, after extensive research, there were no studies that have yet determined the impact of ethical virtues on healthcare organizational outcome of patient satisfaction. In this study, the ethical culture will be measured on the CEV scale (Kaptein, 2008).
Patients report of satisfaction are higher in hospitals where nurses practice in healthy work environments or with more favorable nurse-to-patient ratios, therefore, improving nurse work environments in hospitals could result in improved patient outcomes, including better patient satisfaction (Kutney-Lee et al., 2009). The implication of effective patient communication can potentially lead to increased patient satisfaction. Improved nurse-patient communication would improve quality care, potentially decrease in anxiety, foster safety, and enable patients to develop trust in nursing care, which has the opportunity to lead to increase patient satisfaction (Oni, 2012). Communication with nurses lead the other main four HCAHPS dimensions of responsiveness of hospital staff, pain management, communication about medication, and overall rating. Thus, communication with nurses is a rising tide measure among the eight HCAHPS dimensions of care (Press Ganey, 2013).
It is not known what relationship, if any; exist between ethical culture and patient satisfaction in healthcare organizations. Several researchers examined employees’ perception of ethical culture and its effect on job performance (Huhtalas et al., 2012; Neubert & Roberts, 2013; Wong et al., 2013; Demirtas, & Akdogan, 2015; Riivari & Lasma, 2013; Cohen et al., 2015). However, the perception of healthcare employees of leadership ethical virtues—using the Corporate Ethical Virtues (CEV) model (Kaptein, 2008)—and its relationship to patient satisfaction related to nursing communication have not been explored. There is a need to identify frontline nurses’ perception of leadership ethical culture and examine its relationship to patient satisfaction. The setting for this study will be inpatient units at a large medical center located in a metropolitan area in New York City, New York. Data collection from frontline RNs for this quantitative correlational design study will use the CEV questionnaire (Kaptein, 2008). This design is appropriate for the study because it will design is the most effective methods to investigate the relationship between two or more variables; it provides numerical estimates of the relationship with a comparison of the strength of any identified differences between the two or more variables (Cohen et al., 2011). The independent variable is the frontline employees’ perception of leadership ethics or nursing leadership ethical virtues as measured by the eight dimensions of CEV model. The dependent variable will be patient satisfaction related to nurses’ communications which will measured by the Opinion Meter survey.
The next Chapter is Chapter 3. The purpose of this chapter is to present the methodology that will be used to explore research questions and hypotheses. Additionally, this next chapter will provide an overview of the research design, outline the study population and sampling process, and discuss data collection methods and data analysis procedures. Chapter 3 will also highlight ethical considerations within the study, confidentiality, study location, instrument validity and reliability, and study limitations.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| Chapter 2 Summary This section restates what was written in Chapter 2 and provides supporting citations for key points. The summary section reflects that the learner has done his/her “due diligence” to become well-read on the topic and can conduct a study that will add to the existing body of research and knowledge on the topic. It synthesizes the information from the chapter to define the “gaps” in or “identified research needs” arising from the literature, the theory(ies) or model(s) to provide the foundation for the study, the problem statement, the primary research question, the methodology, the design, the variables or phenomena, the data collection instruments or sources, and the population to be studied. It then provides a transition discussion to Chapter 3. (Minimum one to two pages) | ||||
| Synthesizes the information from all of the prior sections in the Literature Review using it to define the key strategic points for the research. | 2 | 2 | X | |
| Summarizes the gaps and needs in the background and introduction describing how it informs the problem statement. | 2 | 2 | X | |
| Identifies the theory(ies) or model(s) describing how they inform the research questions. | 2 | 2 | X | |
| Justifies the design, variables or phenomena, data collection instruments or sources, and population to be studied. | 2 | 2 | X | |
| Builds a case (argument) for the study in terms of the value of the research and how the research questions emerged from the review of literature | 2 | 2 | X | |
| Reflects that the Learner has done his or her “due diligence” to synthesize the existing empirical research and write a comprehensive literature review on the research topic. | 2 | 2 | X | |
| Summarizes key points in Chapter 2 and transitions into Chapter 3. | 2 | 2 | X | |
| The Chapter is correctly formatted to dissertation template using the Word Style Tool and APA standards. Writing is free of mechanical errors. | 2 | 2 | X | |
| All research presented in the Chapter is scholarly, topic-related, and obtained from highly respected, academic, professional, original sources. In-text citations are accurate, correctly cited and included in the reference page according to APA standards. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Chapter 3: Methodology
Introduction
The purpose of this quantitative study is to explore and analyze the relationship, if any, existing between frontline nursing staff perceptions of their organizational ethical virtues within a health care organization in New York and the impact on organizational outcomes of patient satisfaction. Studies have shown a relationship between ethical culture and organizational outcomes (Yidong & Xinxin, 2013; Neubert, Wu, & Roberts, 2013; Schaubroeck et al., 2012; Kacmar, Carlson, & Harris, 2013; Neubert, Wu, & Roberts, 2013; Demirtas & Akdogan, 2013; Riivari & Lasma, 2013; Sharif & Scandura, 2014; Neves & Story, 2015; Kaptien, 2011, 2016). Ethical leadership influences all levels of hierarchical organizations (Schaubroeck et al., 2011). The topic of ethical culture plays a critical role in organizational innovativeness and subsequent, sustainable performance (Riivari & Lasma, 2013). Studies on the investigation of the relationship between organizational ethical virtues and patient satisfaction related to nurses’ communication are very limited. This study will attempt to identify the potential impact of ethical culture on patient care.
The study proposes a quantitative correlational design utilizing data which will be collected from frontline nursing staff using the demographic questionnaire, Corporate Ethical Virtues (CEV) questionnaire and OpinionMeter, to measure nurses’ communication with patients which is based on the Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) survey. The outcome of this study may position nursing ethics as a critical element of healthcare ethical culture competency and effectiveness.
This chapter contains a discussion of the quantitative methodology and the rationale for the use of a quantitative correlational approach in examining the relationship impact of organizational ethics on patient satisfaction at a healthcare organization in New York City. This chapter includes the statement of the problem, research questions and hypothesis, the research design, population and sampling information, data collection procedures, data analysis techniques, instrumentation validity and reliability, and ethical considerations. This chapter concludes with a summary of the overall methodology.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| CHAPTER 3 INTRODUCTION This section includes both a restatement of the research focus and the Purpose Statement CHAPTER 3 INTRODUCTION (Minimum two to three paragraphs) | ||||
| The introduction restates the purpose statement to the study. This section also outlines the expectations for this chapter | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. |
Statement of the Problem
It is not known what relationship, if any, exists between nursing ethical culture and patient satisfaction related to nurses’ communication in healthcare organizations in a hospital setting is not well-characterized. The objective of this study is to determine whether a relationship exists between organizational ethical virtues and patient satisfaction. An ethical organizational culture promotes working environments that are predicated upon managers’ commitments to organizational goals (Huhtalas, Feldt, Hyvonen, & Mauno, 2012). Ethical leadership has significant influence on an employee’s mindset, behavior, and commitments (Neubert & Roberts, 2013). Relationships can be drawn between the ethical organizational culture and the specific organizational outcomes of organizational innovativeness (Riivari & Lasma, 2013).
Several researchers examined employees’ perception of ethical leadership and its effect on job performance (Demirtas, & Akdogan, 2015; Huhtalas et al., 2012; Neubert & Roberts, 2013; Riivari & Lasma, 2013; Walumbwa et al., 2012; Wong et al., 2013). Work by Demirtas and Akdogan (2015) revealed that ethical leadership is significantly correlated to ethical climate, affective commitment, and turnover intention. However, the finding of this study cannot be generalized to other industries or cultures. The authors recommended conducting further research to consider other organizations culture and include additional outcome variables. Therefore, the proposed study will be focused on other organizational outcome such as patient satisfaction. Further work by Riivari and Lasma (2013) revealed that there is a relationship between ethical organizational culture and specific organizational outcomes and organizational innovativeness. Ethical behaviors of senior management have an important role and effect on organizational innovativeness. The authors suggested conducting further research on ethical leadership related to other group of outcomes such as productivity, efficiency, work satisfaction, and employee commitment. The proposed research will therefore be focused on ethics in nursing and its impact on organizational outcome of patient satisfaction. A study by Huhtalas et al. (2012) revealed that leadership and management practices are important elements related to setting personal work goals. Therefore, the proposed research will explore organizational ethical culture effect on patient satisfaction. Healthcare leaders have considerable influence in the healthcare delivery due to their role and responsibilities. Walumbwa et al. (2012) suggested that ethical leadership can lead to higher in-role performance for groups of staff. The perception of healthcare employees of ethical virtues—using the Corporate Ethical Virtues (CEV) model (Kaptein, 2008)—and its relationship to patient satisfaction related to nursing communication have not been explored. The proposed study will therefore explore whether ethical culture has an impact on patient satisfaction as an outcome.
One sees a continued demand for a sustainable organization culture that promotes quality and patient satisfaction. A viable, organizational ethical culture is essential in establishing the platform for transformation, improvement, and change to meet the demand for quality improvement and patient satisfaction. Therefore, this knowledge could have practical implications for organizational performance and patient satisfaction and quality outcome. Healthy work environments are imperative for the overall nurses’ performance and their ability to communicate effectively with their patients. Hence, it can impact the quality and safety of patient care. Therefore, the need to identify and examine frontline nursing employees’ perceptions of organizational ethical culture is imperative.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| STATEMENT OF THE PROBLEM This section restates the problem for the convenience of the reader. This section is a summary of the related section in Chapter 1. (Minimum one to two paragraphs) | ||||
| The research problem is restated for the convenience of the reader. This section aligns to the related section in Chapter 1. | 2 | 2 | X | |
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | X | |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: Double the problem and ensure it states exactly what the gap is . I was not sure whether what Dr |
Research Question(s) or Hypotheses
It is not known what relationship (if any) exists between ethical culture and patient satisfaction in healthcare organizations. The main research question that will guide this study is whether a relationship can be discerned between organizational ethical virtues and patient satisfaction in a large medical center in New York City. The research is designed as a quantitative study to identify any statistically significant correlation between these variables.
Patient satisfaction is considered an important measure of healthcare delivery. The perception of discharged patients regarding their hospital experience influences their views and opinions with respect to the quality of care that was experienced during their hospitalization. The key questions ascertained within the HCAHPS are the ratings of communication with doctors, communication with nurses, responsiveness of hospital staff, pain management, communication about medication, discharge information, cleanliness of the hospital environment, quietness of hospital environment, and transition of care (CMS, 2013). The Opinion Meter was developed to measure patient experience based on the HCAHPS which is patient interaction during healthcare encounter. Nurses are the backbone and the face of the patients’ daily care; therefore, nurses’ communication can impact the overall patient satisfaction and the likelihood to recommend the hospital. Hence, active nursing communication and sharing information with patients are a venue to improve patient satisfaction. The aspects of nursing care and communication are more predictive of patient satisfaction than interactions with physicians, and represent the factors that influence overall patient-experience scores in hospital settings (Manary, Boulding, Staelin, & Glickman, 2013). Nursing is a therapeutic approach to patient care. Hence, the relationship between the nurse and the patient is therapeutic and based on trust and mutual understanding, open communication, and the fostering of mutual goal setting (Peplau, 1997). Improved nursing staff communication skills should eventually increase patient satisfaction (Oni, 2012).
The independent variable is the frontline employees’ perceptions of leadership ethics as measured by the eight dimensions of the CEV Model which include clarity, congruency of supervisor and congruency of management, feasibility, supportability, transparency, discussability, and sanctionability. The dependent variable will be patient satisfaction as measured by the OpinionMeter which based on one item from the HCAHPS survey that relates to nurses’ communication with patients. Other statistical covariates include registered nurses’ demographic information which includes sex, age, education, race years of service and primary shift. The data will be collected from a sample of 128 frontline nursing staff through an online survey. The variables for this study were selected to address the following research questions and hypothesis:
RQ1: Is there is relationship between organizational ethical culture and patients’ rating of communication with nurses?
H1: Organizational ethical culture is positively related to patients’ rating of communication with nurses.
H01: Organizational ethical culture is not related to patients’ rating of communication with nurses.
RQ2: Is there is relationship between the dimension of clarity and patients’ rating of communication with nurses?
H2: Clarity is positively related to patients’ rating of communication with nurses.
H02: Clarity is not related to patients’ rating of communication with nurses.
RQ3: Is there is relationship between the dimension of congruency of supervisor and patients’ ratings of communication with nurses?
H3: Congruency of supervisor is positively related to patients’ rating of communication with nurses.
H03: Congruency of supervisor is not related to patients’ rating of communication with nurses.
RQ4: Is there is relationship between the dimension of congruency of management and patients’ rating of communication with nurses?
H4: Congruency of management is positively related to patients’ rating of communication with nurses.
Ho4: Congruency of management is not related to patients’ rating of communication with nurses.
RQ5: Is there is relationship between the dimension of feasibility and patients’ rating of communication with nurses?
H5: Feasibility is positively related to patients’ rating of communication with nurses
Ho5: Feasibility is not related to patients’ rating of communication with nurses
RQ6: Is there is a relationship between the dimension of supportability and patients’ rating of communication with nurses?
H6: Supportability is positively related to patients’ rating of communication with nurses
Ho6: Supportability is not related to patients’ rating of communication with nurses
RQ7: Is there is a relationship between transparency and patients’ rating of communication with nurses?
H7: Transparency is positively to patients’ rating of communication with nurses
Ho7: Transparency is not related to patients’ rating of communication with nurses
RQ8: Is there is a relationship between the dimension of discussability and patients’ rating of communication with nurses?
H8: Discussability is not related to patients’ rating of communication with nurses.
Ho8: Discussability is positively related to patients’ rating of communication with nurses.
RQ9: Is there is a relationship between the dimension of sanctionability and patients’ rating of communication with nurses?
H9: Sanctionability is positively related to patients’ rating of communication with nurses.
Ho9: Sanctionability is not related to patients’ rating of communication with nurses.
This study may offer support and necessary information for healthcare organizations to assess the impact of ethical virtues as perceived by frontline nursing staff on patient satisfaction. Patient satisfaction is one organizational outcome of patient ratings of their experience with the staff that care for them. The findings of this study could provide recommendations, teaching tools, programs, and lead to strategic planning and change in order
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| RESEARCH QUESTIONS AND/OR HYPOTHESES (Minimum one to two pages) | ||||
| Qualitative Studies: Restates the research questions and the phenomena for the study from Chapter 1. Quantitative Studies: Describes the variables, at the conceptual, operational and measurement levels, then restates the research questions from Chapter 1, and presents the matching hypotheses. | 2 | X | ||
| Describes the nature and sources of necessary data to answer the research questions (primary versus secondary data, specific people, institutional archives, Internet open sources, etc.). Quantitative Studies: Describes the data collection methods, instrument(s) or data source(s) to collect the data for each variable. Qualitative Studies: Describes the data collection methods, instruments, and/or data sources to collect the data to answer each research question. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | X | |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
to improve the organizational patient experience.
Research Methodology
This study will use quantitative methodology to collect and analyze numeric data. This type of systematic approach enables the researcher to collect information and subsequently transform the evidence into numerical data. The researcher will be testing the hypotheses identifying statistical relationships between variables. This study will use a quantitative methodological approach to investigate whether or not there is a significant different inpatient satisfaction with nurses’ communication at a healthcare organization in New York City between medical and surgical nursing units when controlling for nurses’ leadership ethical virtues. Studies of ethical leadership have utilized both quantitative and qualitative methods (Brown et al., 2005). In quantitative research, the investigator believes that the reality is objective and controlled by cause and effect relationships (Arghode, 2012). Quantitative research is known by objectivist epistemology and seeks to develop explanatory universal laws in social behaviors by statistically measuring what is assumed to be static reality (Yilmaz, 2013).
Quantitative researcher employ the use of numbers to study the phenomenon or occurrence, and the researchers are usually outsiders who do not influence the outcome of the quantitative research. Quantitative methodology focuses on proving or disproving a hypothesis based on large numbers of participant responses (Arghode, 2012). The idea is also to generalize results onto larger populations by conducting analysis using sophisticated statistical tools (Arghode, 2012). The quantitative survey research method was preferred for gathering the data over the qualitative research method in that qualitative studies are non-numerical and assume that one may encounter multiple and subjective realities. A quantitative approach endorses the view that psychological and social phenomena have an objective reality. Hence, reality should be studied objectively by the researcher with some distance between themselves and what is being studied.
Unlike quantitative studies which are concerned with outcomes, generalization, prediction, and cause-effect relationships through deductive reasoning, qualitative studies are concerned with process, context, interpretation, meaning or understanding through inductive reasoning (Yilmaz, 2013). The qualitative interview method also requires personal contact with each study participant. The cost in funds and time to obtain data from a significant sample size of 128 frontline nursing staff, using the interview method would have been too high for the research budget. In the case of this study, quantitative methodology was chosen in an effort to statistically analyze the relationship between ethical culture and patient satisfaction.
The first main variables of this study are frontline employees’ perception of leadership ethics as measured by the CEV model, which include: clarity, congruency of supervisor and management, feasibility, supportability, transparency, discussability, and sanctionability. The dependent variable will be patient satisfaction related to nurses’ communications which will measured by the OpinionMeter which is based on the Hospital-Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. Through the OpinionMeter, the study will use one item from the HCAHPS survey which relates to nursing: communication with nurses. Other variables included demographics data. These include the respondents’ (Registered nurses) sex (male/female), age (years), education (degree), race, years of service, and primary shift. The quantitative survey instrument for this research will ensure that the survey questions will be asked in a clear, concise and consistent manner through an online survey for each participant.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| RESEARCH METHODOLOGY (Minimum one to two pages) | ||||
| Provides a rationale for the research methodology for the study (quantitative, qualitative, or mixed) based on research books and articles. | 2 | X | ||
| Provides a rationale for the selected the methodology based on empirical studies on the topic. | 2 | |||
| Justifies why the methodology was selected as opposed to alternative methodologies. | 2 | |||
| Uses authoritative source(s) to justify the selected methodology. Note: Do not use introductory research textbooks (such as Creswell) to justify the research design and data analysis approach. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Research Design
A quantitative correlational study will serve as the research design for this research. Researchers use correlational design when they want to examine the relationships between variables. This study will use a correlational approach to provide a different perspective, which also reduced the personal bias often found through the gathering and analysis of qualitative data (Gay et al., 2011). A correlational study, regardless of the significance of the findings, does not imply causation, but shows a relationship between variables (Polit & Tatano-Beck, 2012). A correlational research design will be used for this study because of its ability to measure the degree of association between variables, not which one causes a change in the other (Gay et al., 2011). The variables in the current study will not be manipulated or controlled; therefore, a correlation design is appropriate for this study. The correlational design strategy will be explicit to a specific sample from a population, which are frontline nursing staff. The empirical data of this study will be collected through an online questionnaire, which will be distributed to frontline nursing staff. The purpose of the correlational design study is to establish the degree to which a relationship exists between variables (Gay et al., 2011).
Unlike causal-comparative, experimental, truth tables, case studies and other study designs, using correlations in this study was more appropriate because of the calculation of the net effect of two variables. In addition, the use of formulae in correlational studies helped in manipulating variables to establish the nature of the bivariate relationships (Ragin, 2014). The quantitative correlational research design was the most appropriate method for accomplishing the goals of this study because it involves the collection, tallying and logical collation of quantities of data to examine possible relationships between variables. It was appropriate for the current research that studied relationship between variables. Therefore, correlational design is optimal for this study because the objective is to investigate the relationship between nursing leadership ethical virtues and patient satisfaction.
Pearson product moment correlation coefficient will be computed in order to determine the degree and the direction of the relationship between the variables based on the recommendations that the test has been shown to be robust with regard to somewhat non-normal distributions (Laerd, 2013). Pearson’s correlation determines the degree to which a relationship is linear, it determines whether there is a linear component of association between two continuous variables. Correlation coefficients are used to assess the strength and direction of the linear relationships between pairs of variables. When both variables are normally distributed, Pearson’s correlation coefficient is more appropriate than Spearman’s correlation coefficient (Mukaka, 2012). Correlation coefficients do not communicate information about whether one variable moves in response to another. In this study, there is no attempt to establish one variable as dependent and the other as independent. Thus, relationships identified using correlation coefficients should be interpreted for what they are: associations, not causal relationships. The Pearson correlation determined r values (correlation coefficients) for the study variables with values ranging between +1 to -1 with values near the 0 point indicating no correlation, values near +1 indicating a strong positive relationship, and values near -1 indicating a strong negative relationship.
Quantitative data will derive from the CEV scale measurements and OpinionMeter survey scores. The variables of this study are nursing ethics as measured by the CEV Model which include: clarity, congruency of supervisor and management, feasibility, supportability, transparency, discussability, and sanctionability. The second main variable of patient satisfaction related to nurses’ communication will be measured by the OpinionMeter. Other variables included background variables will include the respondents’ (Registered nurses) sex (male/female), age (years), education (degree), race, years of service and primary shift. This study will focus on the influence of nursing perception of ethical culture on certain organizational outcome in a hospital medical surgical nursing unit, with particular focuson the scores of communication with nurses. Accordingly, the unit of analysis will be both staff nurses and their assigned patients. Frontline nursing staff with at least one-year of experience who is involved in direct patient care in an inpatient hospital setting.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| RESEARCH DESIGN (Minimum one to two pages) | ||||
| Elaborates on the research design from Chapter 1. Provides the rationale for selecting the research design supported by empirical references. Justifies why the design was selected as the best approach to collect the needed data, as opposed to alternative designs. | 2 | X | ||
| Quantitative Studies: Provides the variable structure and states the unit of analysis. and unit of observation. If multiple data sources have different units of observation, specify the key variable for matching cases. Qualitative Studies: Provides the unit of analysis and the unit of observation. If multiple data sources have different units of observation, specify the matching cases. In qualitative study designs the units of analysis (or observation) are each sample participant. In case study design (single or multiple), the unit of analysis is a “bounded system” in its own right. This could include one individual, one family, one group, one community, one school, one policy, one region, one state, one country, etc. The sample may include several participants, but these must be members of a homogeneous unit representing the “bounded system” that is the case study unit. | 2 | |||
| Uses authoritative source(s) to justify the design. Note: Do not use introductory research textbooks (such as Creswell) to justify the research design and data analysis approach. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Population and Sample Selection
The setting for this study will be inpatient units at a large medical center located in a metropolitan area in New York City, New York. The medical center offers a wide range of services and includes a 650-bed capacity, full-service hospital with trauma, emergency, medical-surgical, critical care, obstetric, pediatric, psychiatry, cardiovascular, and critical care services. The medical center have a base of 6,500 employees, of which 1,040 are staff RNs who work in a variety of settings, such as medical-surgical units, behavior health units, intensive care units, the emergency room, and outpatient services. The hospital employs only a few licensed practical nurses (LPNs) and approximately 700 unlicensed support staff including patient care associates (PCAs) and patient care technicians (PCTs). However, the current study will focus only on the 200 medical and surgical registered nurses (RNs) in the inpatient units; however, other units and the outpatient staff will not be included. The patient population will include patients covering all socioeconomic strata within the New York metropolitan area. The nursing leadership structure at the study healthcare organization consists of a chief nursing officer (CNO) who is responsible for system-wide nursing operations and provides overall nursing leadership guidance for the organization. Nursing leadership will include assistant directors of nursing (ADNs), associate directors of nursing (ADONs) and directors of nursing (DONs). The study population will include all frontline staff RNs working on the inpatient units. However, head nurses or those with titles of manager or director will be excluded. Accordingly, the study will be limited to frontline nursing staff with at least one-year experience who involved in direct patient care in an inpatient hospital setting.
Participants of this study will be recruited solely on their willingness to participate. To determine the appropriate sample size for the target population, the researcher conducted a power analysis to determine the minimum sample size. The sample size was determined based on the number of inpatient registered nurses (RN’s). The size of a probability (random) sample can be determined by using a power analysis using G*power. G*Power is a stand-alone power analysis software, used for various statistical tests (Peng, Lomg, & Abaci, 2012). Prior research suggests that a medium size effect is expected in the present research. So, the input parameters for one regression are an adjusted medium effect size of 0.25, an alpha of 0.05, a power of 0.80, and eight dimensions for nursing ethical virtues will result in a computation of a minimum sample size of 128 (Appendix A) as the number representative of the total sample size.
To be eligible, participants will have to be licensed as registered nurses in an inpatient unit, and must have been in the current position for at least one year. The chief nursing officer and other nurse administrators of the healthcare organization in New York City will be informed of the study details and purpose to gain adequate knowledge of the study procedures, allowing support for the study, and solicitation of ideas as to which units would be appropriate for the study. A letter of the study approval will be obtained from the research site. The research study proposal was submitted to the hospital Institutional Board Review (IRB) prior to the start of the study. Participants confidently will be maintained. Prior to collection of data, informed consent will be obtained (Appendix C), and a letter contained a detailed explanation of the research study through a link and password to the CEV questionnaire (Appendex E) will be provided. The OpinionMeter will be measuring nurses’ communication and it will be administered to patients on a electronic hand device. The survey will be administered to patients than are link to the same nurse. The patient will rate the nurse in four categories: never, sometimes, usually, or always (Appendix G). A meeting will be conducted with the nurse managers and frontline staff of the participating units to provide forums of communication on the intent of the study and to explain the study procedures and answer questions.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| POPULATION AND SAMPLE SELECTION (Minimum one to two pages) | ||||
| Describes: The population of interest (The group to which the results of the study will be generalized or applicable) (such as police officers in AZ), The target population from which the sample is selected (such as police officers in AZ who belong to the police fraternal association). The study sample (individuals drawn from target population who provide final source of data) (final number from whom complete data were collected). | 2 | X | ||
| 1. Site Authorization and Recruitment 2. Describes the process for obtaining site authorization to access the target population. 3. Describes the site authorization process (what needs to be included in request) confidentiality measures, study participation requirements, and geographic specifics. 4. If public data sources or social media are used to collect data, although site permission is not required, provide arguments and evidence as to why these sources can be used without site permission. 5. Describes the sampling strategy and process for recruiting individuals to comprise the sample. | 2 | |||
| Quantitative Sample Size Requirements Describes the expected study sample and the proposed and rationale: An a priori or equivalent analysis and/or post hoc Power Analysis is required to justify the study sample size based on the anticipated effect size and selected design. Certain procedures are applicable for small samples. Those situations must be justified through computation or literature. Justification is based on the selected design and statistical procedures. G*Power or equivalent computation is required. G*Power software can be downloaded from the link presented below https://www.gpower.hhu.de/en.html using an alpha error of 0.05, a medium effect size and statistical power of 0.80 for each statistical analysis that is proposed.” | 2 | X | ||
| When calculating the expected return rate for questionnaires and surveys, assume the return rate is 5-10% when no incentives are provided and 15-20% when incentives are provided. Attrition: When doing repeated measures studies in an experiment, learners should consider probable loss to attrition. Qualitative Sample Size Requirements: The sample size should be stated for each form of data collection including interviews, observations, questionnaires, documents, artifacts, visual data such as drawings and photographs, etc. Case Study: Guideline: A minimum of 10 participants or cases in the final sample for interviews. Learners should pursue a minimum 20 individuals to recruit to account for attrition; minimum of three sources of data; must demonstrate triangulation of the data across two sources for each RQ. Case study interviews may include closed-ended questions with a dominance of open-ended questions; should be no less than 30 minutes; no less than five pages of participant responses/speech in the transcribed data per interview, single spaced, 12 pt. Times New Roman. A minimum of 50 questionnaires if the questionnaires will be used for thematic analysis. The size for other sources (e.g., number of documents or artifacts, observations, etc. should also be identified. Phenomenology: Guideline: Minimum of 8 interviews. Learners should pursue 12 individuals to interview to account for attrition. Interviews should be 60-90 minutes. There should be no less than 12 pages of transcribed data, single spaced, 12 pt. Times New Roman, per interview. Interview questions must be open-ended. Descriptive: Guideline: A minimum of 10 participants in the final sample. Learners should pursue a minimum 20 individuals to recruit; 2 sources of data; no less than 5 pages of transcribed data, single spaced, 12 pt. Times New Roman, per interview. Narrative: Purpose is a collection of stories around a phenomenon. Protocol offers questions that get the participant to tell their personal story regarding a phenomenon including the roles of stakeholders. Guideline: Minimum of 8 interviews. Learners should pursue 12 participants to account for attrition. Interviews should be 60-90 minutes. There should be no less than 12 pages of transcribed data, single spaced, 12 pt. Times New Roman, per interview. Interview questions must be open-ended. Note: A key criterion for selecting a sample size for a narrative study is to elicit long, in-depth of stories about the phenomenon which may be hours long. Grounded Theory: Grounded theory studies yield a theory or model. Usually two rounds of data collection with interim analysis. Minimum of 50 pages of transcribed data from interviews, open-ended questionnaires, or other data sources. Transcripts are 12point font and single spaced. Studies typically have a minimum of 10-30 interviews (45-60 minutes in length) and/or 40-60 open-ended questionnaires. Interview questions must be open-ended. Questionnaires or Surveys: If used in the study the minimum number should be 40. This data collection method can be used in different qualitative designs. | 2 | |||
| Strategies to account for attrition: Students should consider the anticipated sample size will not be reached, so must provide a justification or alternative plan for the study (expanding time frame, expanding target population, changing design to bring down sample size needed, or adding an additional data collection approach, adjust an analysis). | 2 | |||
| Defines and describes the sampling procedures (such as convenience, purposive, snowball, random, etc.) supported by scholarly research sources. Includes discussion of sample selection, and assignment to groups (if applicable), and strategies to account for participant attrition. For a purposive sample identify the screening criteria and device for screening the participants (egg: demographic questionnaire, expert knowledge of topic, screening questions such as years of experience in a position). | 2 | X | ||
| Describes the study sample size. Provides evidence (based on the empirical research) literature that sample size is adequate for the research design and meets GCU required sample size requirements (listed in criteria below). | 2 | |||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Instrumentation
There are many instruments designed to directly measure ethical leadership and ethical culture; the ethical leadership survey (Brown et al, 2005); the perceived leadership integrity scale (Craig & Gustafson, 1998); the ethical leadership work (ELW) questionnaire (DeHoogh & Den Hartong, 2008), and the corporate ethical virtues (CEV) survey. The proposed study will be based on the CEV model. The ethical virtues will be measured using the 58-item Corporate Ethical Virtues (CEV) questionnaire developed by Kaptein (2008). The participants will rate the 58-item CEV questionnaire on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). Patient ratings of communication with nurses will be measured through the Opinion Meter which is based on the Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS). The CEV was chosen because it is a valid survey instrument that captures the eight dimensions of ethical virtues. This questionnaire will be assessing the nurses’ perception of their organization’s ethical virtues. This study will be focused on organizational ethical culture impact on nurses’ communication and overall patient satisfaction.
The structure of the CEV scale for measuring and evaluating ethical culture has been previously tested and validated by various researchers using Dutch and Finnish data (Huhtala et al., 2011; Kaptein 2008). Furthermore, Kaptein (2011) study used the CEV scale in a large sample of U.S. employees in fifteen selected industries. The CEV scale consists of 58 items that comprise eight dimensions of organizational virtues: (1) Clarity (ten items); (2) Congruency of supervisor (six items; (3) Congruency of management (four items); (4) Feasibility (six items); (5) Supportability (six items); (6) Transparency (seven items); (7) Discussability (ten items); and (8) Sanctionability (nine items; Kaptein, 2008).
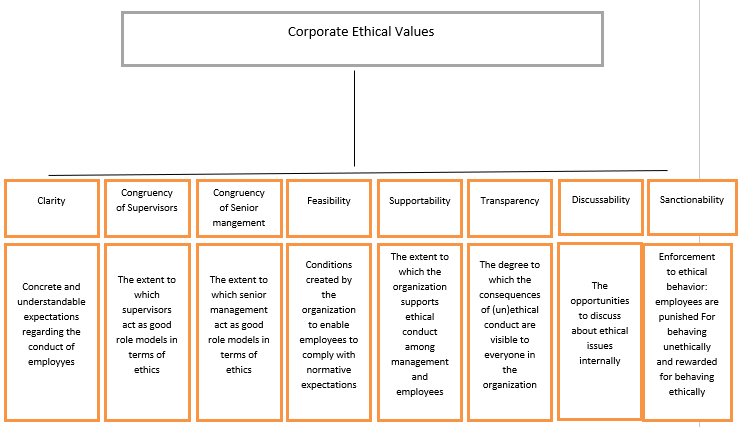
Findings from previous studies supported both the construct and criterion validity of the scale, and the reliability of the different dimensions was also found to be high. Previous studies concluded that the CEV scale provides a reliable and valid instrument for investigating ethical dimensions, and these virtues reflect the quality of the ethical culture in different organizational settings (Huhtala et al., 2011; Kaptein, 2008). For this study, the covariates of leadership ethical virtues will include eight measures using the different dimensions of the CEV scale. The average scores of the question items measuring each of the CEV dimensions were obtained to measure the eight measures of the covariate of leadership ethical virtues. This makes the measure of the covariate of leadership ethical virtues as a continuous measured variable. Riivari, Lämsä, Kujala and Heiskanen (2012) tested the eight variables of the CEV model. Cronbach’s α‘s were above 0.843, which suggests that all dimensions have relatively high internal consistency.
The dependent variable of patient satisfaction related to nurses’ communication will be measured by the Opinion Meter which is based on the HCAHPS survey. The version of the HCAHPS survey instrument is comprised of 32 care items. Included are 22 questions that focus on nine main topics: Communication with nurses, communication with the doctors, responsiveness of hospital staff, pain management, communication regarding medication, discharge information, hospital environment (cleanliness), hospital quietness and transition of care (Cons, 2013). The HCAHPS is a standardized survey instrument that measures patients perception of their hospital stay and experience. The predictive validity of a patient satisfaction instrument (HCAHPS) can be estimated by the degree to which individual items on the instrument predict the patients’ intentions to recommend. In this regard, the questionnaire shows high levels of predictive validity. A series of simple regression analyses revealed that each of the individual items is a significant predictor (at the .001 level) of a patient’s reported likelihood to recommend the facility (beta’s ranged between .35 and .85).
For this study, the dependent variable is the patient satisfaction related to nurses’ communication measured through the Opinion Meter using one item from the HCAHPS survey which measures communication with nurses. The patient satisfaction with nurses’ communication are measured with three rating questions and these include “Nurses treat with courtesy/respect”; “Nurses listen carefully to you”; and “Nurses explain in way you understand”. The average score of the three question items will be used to measure patient satisfaction with nurses’ communication. . The patient will rate the nurse in four categories: never, sometimes, usually, or always (Appendix G).
Lastly, basic demographic data which include the following items: (Registered nurses) gender (male/female), age (years), education (degree), race, years of service and primary shift, and the CEV scale of ethical culture.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| RESEARCH MATERIALS, INSTRUMENTATION, OR SOURCES OF DATA (Minimum one to three pages) | ||||
| Data Collection Instruments/Materials: Provides a detailed discussion of the instrumentation and/or materials for data collection which includes validity and reliability of the data. collection instrument or experiment. Includes citations from original publications by instrument developers (and subsequent users as appropriate) or related studies. | 2 | X | ||
| Data Collection Instruments/Materials: Describes the structure of each data collection instrument and data sources (tests, questionnaires, interviews, observations data bases, media, etc.). When using materials for an experiment, describes the structure of the experiment and the materials used for it. Specifies the type and level of data collected with each instrument. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Validity
Validity is the degree to which a questionnaire measures what it was designed to measure. Validity provides the basis for drawing useful and meaningful inferences from scores on a particular research instrument (Cozby & Bates, 2015). The ethical culture of organizational leadership was measured with the CEV questionnaire (Kaptein 2008). The CEV model was validated through four empirical studies by Kaplein (2008) The internal consistencies for each factor were high, with Cronbach’s alphas ranging from 0.93 to 0.96. In addition, the CEV scale was validated by Riivari et al. (2012) which showed that the eight dimensions of the CEV model Cronbach’s α‘s are above 0.843 which suggested that all dimensions have relatively high internal consistency.
Evidence of convergent validity of the eight dimensions of the CEV has been supported by prior reseach (Kaptien, 2008; Huhtala et al., 2011; Kangas et al., 2013). The study of Huhtala et al. (2015) showed support for the criterion validity of the model because the amount of shared variance differed for each eight dimensions at the work unit level.
The internal consistency coefficients scores (0.68- 0.89) of the study of Miltonga–Monga and Cilliers (2015) showed acceptable reliability coefficient CEV scale. Novelskaite and Pucetaite (2014) analysis of the CEV model also showed internal coefficients scores (0.68-0.89) and suggested that it can be valid for Lithuanian sociocultural context but with some limitation due to insufficient clarity in the Lithuanian data analysis of the mixed loadings of the virtues such as Discussability, Transparency, Supportability or Sanctionability. In addition, longitudinal validity has been examined in one study over two-time periods which revealed that the eight–dimensional factor structure of the CEV scale is invariant as a function of time (Huhtala, Kaptein, & Feldt, 2015). The CEV scale was validated in different cultures, organization, and groups and the main strength of this model is that can provide a strong basis for interventions around the CEV virtues. Therefore, the proposed research will conceptualize ethical culture by using the 3 items from the CEV model (Kaptien, 2008) to examine the relationship between nursing leadership ethical culture in health organization and patient satisfaction related to nurses’ communication.
The predictive validity of a patient satisfaction instrument (HCAHPS) can be estimated by the degree to which individual items on the instrument predict the patients’ intentions to recommend. In this regard, the questionnaire shows high levels of predictive validity. A series of simple regression analyses revealed that each of the individual items is a significant predictor (at the .001 level) of a patient’s reported likelihood to recommend the facility (beta’s ranged between .35 and .85). Additionally, multiple regression analyses revealed that, collectively, all items are significant predictors of patient’s reported experiences (Press Ganey, 2013).
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | |
| VALIDITY (for Quantitative Studies)/TRUSTWORTHINESS (for Qualitative Studies) (Minimum two to four paragraphs or approximately one page) | ||||
| Quantitative Studies: Provides specific validity statistics for quantitative instruments, identifying how they were developed. Validated surveys cannot be used in part or adapted. Validated instruments borrowed by the learner must be included in the proposal/dissertation appendices as a pdf or jpeg document along with the learner’s word file of his/her version of the instrument (whose content should be identical with that of the original pdf). NOTE: Learners should not modify or develop quantitative instruments without permission from the Director of Dissertations. Qualitative Studies: Trustworthiness is the term used to describe the elements that establish the credibility, transferability, dependability, and confirmability of the study. Strategies generally include rigorous techniques and methods, thick description, audit trails, evident methodological processes and procedures, well-defined coding, ample examples of quotes, and findings that clearly emerge from the data. | 2 | X | ||
| Appendices must include copies of instruments, materials, qualitative data collection protocols, codebooks, and permission letters from instrument authors (for validated instruments, surveys, interview guides, etc.) | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Reliability
Reliability testing is a method of evaluating the internal consistency of a questionnaire. The traditional statistic used to illustrate the degree of consistency among the items of a scale or questionnaire is Cronbach’s alpha. A set of questions with no internal consistency—no reliability—has an alpha of 0.0 indicating that the questions within the scale may not be measuring the relevant issues. A set of questions with perfect internal consistency has an alpha value of 1.0. All ten scales exceeded the stringent .70 standard for reliable measures. Cronbach alpha scale reliability was performed for the eight virtues of ethics: Clarity .93, Congruency of supervisors, .95, Congruency of management, .95, Feasibility, .96, Supportability, .95, Transparency, .93, Discussability, .94, and Sanctionability, .94. The overall fit of the model is quite high.
The corporate ethical virtues (CEV) model was developed by Kaptein (1998, 1999). The study of Kaptein (2008) validated and refined the model. An exploratory factor analysis was performed and provided support for the existence of eight unidimensional corporate ethical virtues: clarity, congruency of supervisors, congruency of management, feasibility, supportability, transparency, discussability, and sanctionability. Item reliabilities ranged between .93 and .96 and produced strong evidence supporting the convergent and discriminant validity of the structure of the CEV scale (Kaptein, 2008).
When using Likert-type scales one must calculate and report Cronbach’s alpha coefficient for internal consistency reliability for any scales or subscales one may be using. The analysis of the data then must use these summated scales or subscales and not individual items. If one does otherwise, the reliability of the items is at best probably low and at worst unknown (Gliem & Gliem, 2003). According to Cohen, Manion and Morrison (2013), reliability coefficients between 0.60 and 0.80 are acceptable. The study of Mitonga-Monga and Cilliers (2015) showed an acceptable reliability coefficient for the CEV scale. Thus, the internal consistency coefficients of scores from the CEV for the study sample ranged from 0.68 to 0.89. The factorial structure of the 58-item CEV scale has been found to be very good in a Finnish sample of public sector employees (Kangas et al., 2014). The reliability coefficient of the CEV scale was reported between 0.83 and 0.96. The lowest values were found for feasibility (between 0.80 to 0.88) and the highest values for congruency of supervisors (between 0.95 to 0.97). The results of the 58 item, self-reporting questionnaire is a useful tool and can be used in future research to assesss ethical culture (Kaptien, 2008).
HCAHPS’ reliability ranged from .78 to .95 (Press Ganey, 2013). The Cronbach’s alpha for the entire questionnaire is .97, confirming the instrument’s high internal consistency and reliability. The inpatient instrument was found to be psychometrically sound across a wide variety of tests of validity and reliability. The scales for communication with doctors, communication with nurses, and pain management showed relatively consistent reliabilities that remained above the .70 benchmark. The measures of communication about medicines, discharge information, and responsiveness of hospital staff showed poor reliabilities. Therefore, these measures need further scrutiny and refinement before they are used for financial considerations (Westbrook, Babakus, & Grant, 2014).
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| RELIABILITY This section describes and defends the procedures used to determine the reliability of the data collected appropriate to the methodology conducted. (Minimum two to four paragraphs or approximately one page) | ||||
| Quantitative Studies: Provides specific reliability statistics for quantitative instruments, identifying how the statistics were developed. Explains specific approaches on how reliability will be addressed for qualitative data collection approaches. Qualitative Studies: Establishes consistency and repeatability of data collection through in-depth documented methodology; detailed interview/observation/data collection protocols and guides; creation of research data-base; and/or use of triangulation. | 2 | 2 | 2 | X |
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | 2 | 2 | X |
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Data Collection
Following the approval of Institutional Review Board (IRB) to collect data and site authorization from one organization in New York City, participants will receive a letter of invitation to participate in the online-administrated survey. The data will be collected in one healthcare organization, which consists of 5,500 employees. There is a total of 885 frontline staff in the inpatient units. A sample will be selected from total target employees of 200 frontline nursing staff from the medical surgical units. For each participant, data will be collected from their assigned patient.
Data collection for this quantitative correlational study will use electronic administration of the questionnaires that were accessed through a regular internet connection. Survey Monkey will be used to a collect data. Data collection for this study will be conducted after the proper IRB approval through Grand Canyon University. Once permission is granted to initiate the process, a letter will be given to the healthcare organization to receive hospital approval to conduct research. A meeting will be held with the chief nursing officer and other nurse administrators to describe the purpose and design of the study as well as the ethical standards of confidentiality.
Two weeks before launching the survey, the chief nurse executive will send a memo to all members of the target population of 200 RNs for the study. The memo will contain an explanation of the research, including its purpose, nature, and process. The memo will be state that the participation in the study will be voluntary. The data collection will not identify individual participants. Informed consent will be obtained from all participants using the informed consent template of GCU (Appendix D).
Prior to collection of data, informed consent will be obtained, and a meeting will be conducted with the nurse managers and frontline staff of the participating units. Forums will be used to communicate the intent of the study, explain the study procedures, and answer questions. Participants will rate the 58-item CEV questionnaire on a Likert scale from 1 (strongly disagree) to 5 (strongly agree) to measure the independent variables of ethical virtues. The researcher will create Survey Monkey survey that includes electronic versions of all the questions asked in the study. The dependent variable of patient satisfaction related to nurses’ communication will be collected from the patients that assigned to the same nurses, through the Opinion Meter which based on the HCAHPS survey (Appendix G)
The data will be collected from a sample of 128 inpatient registered nurses (RNs). Head nurses and support staff will be excluded. A meeting will be conducted with the nursing staff to inform them about the purpose of the research, and the benefits of participating. Demographic questions include age, gender, length of experience, age, race, education level, and primary shift worked will be used to gather information about the participants. Data will be kept securely in the database accessible via password to the researcher. Timelines will be established to maintain the collection of data and to conclude the data collection portion of the study at a specifically stated date. Questionnaire access will be closed at the stated expiration. However, if necessary, access will be extended to ensure that the required number of participants has been met. The participant will be given 24/7 access to the survey site for a period of 14 days. If necessary, time will be extended to improve response rates. Intermittent reminders will be sent to the participants via email. The researchers will remind the participants to answer the questions to the best of their ability and to be honest about their responses in each section of the survey. Participants will be asked to return the informed consent prior to participation, and then will be allowed to proceed to the link from Survey Monkey®.
The participants will be given an informed consent/request letter form describing the request to participate in the study, purpose of the survey, confidentiality of information, and the means to return the survey to the researcher anonymously. The individual participants’ informed consent will be downloaded to the CEV survey site. The patient satisfaction survey will be collected through the Opinion Meter. The collected data will be stored securely in electronic form which is only accessible to the researcher that administrates the study. This data collection will not identify individual participants. Data will be thoroughly analyzed and disaggregated to support the obligations of the study. The data will be destroyed after a period of three years per Grand Canyon University IRB procedure, via deletion of the database.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| DATA COLLECTION AND MANAGEMENT (Minimum one to three pages) | ||||
| Quantitative Studies: Describes the procedures for the actual data collection that would allow replication of the study by another researcher, including how each instrument or data source was used, how and where data were collected, and recorded. Includes a linear sequence of actions or step-by-step of procedures used to carry out all the major steps for data collection. Includes a workflow and corresponding timeline, presenting a logical, sequential, and transparent protocol for data collection that would allow another researcher to replicate the study. Data from different sources may have to be collected in parallel (e.g., paper-and-pen surveys for teachers, corresponding students, and their parents AND retrieval of archival data from the school district). A flow chart is ok—”linear” may not apply to all situations Qualitative Studies: Provides detailed description of data collection process, including all sources of data and methods used, such as interviews, member checking, observations, surveys, and expert panel review. Note: The collected data must be sufficient in breadth and depth to answer the research question(s) and interpreted and presented correctly, by theme, research question and/or instrument. | 2 | X | ||
| Describes the procedures for obtaining participant informed consent and for protecting the rights and well-being of the study sample participants. Include site authorization letter(s) and participants’ informed consent (parents’ consent and children’s consent, as needed) in appendices. | 2 | X | ||
| Describes how raw data are prepared for analysis (i.e., transcribing interviews, conducting member checking, downloading from SPSS and checking for missing data). Describes (for both paper-based and electronic data) the data management procedures adopted to maintain data securely, including the length of time data will be kept, where it will be kept, and how it will be destroyed | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Data from surveys will be collected from frontline nursing and analyzed to measure their perceptions of ethical organizations. Data regarding patient satisfaction related to nurse’ communication will be collected from the patient that were assigned to the same nurse through the OpinionMeter. The data will be analyzed to determine to what degree a relationship exists between organizational ethical culture and patient satisfaction at a healthcare organization in New York City.
Data management and statistical analyses will be performed using Microsoft Excel version and the IBM statistical package for social services (SPSS) ® software. The data from surveys will be exported from Microsoft excel to SPSS. The nature of the variables, the research questions, and prior research guided the most appropriate statistical analysis. The eight dimensions of the ethical virtues will be the independent variables; patient satisfaction related to nurses’ communication will be the dependent variable.
Data will be analyzed and summarized using descriptive statistics. Descriptive analysis can provide maximum and minimum values, distribution, average, and mean of both independent and dependent variable ( Greavetter &Forzano, 2015). The researcher will complete subscales and scales and will also create a frequency table of the number and demographics of respondents. Frequencies and percentage tables will be analyzed for categorical or nominal measured variables, while descriptive statistical measures of means and standard deviations will be used to summarize the data for variables that are continuously measured. Scatterplots will be inspected for violations of statistical assumptions. Ethical culture will be collected from frontline nursing staff through the online survey. Satisfaction with nurses ‘communication will be collected from patient through the OpinionMeter. The variables for this study were selected to address the following research questions and hypothesis:
RQ1: Is there a relationship between organizational ethical culture and patients’ rating of communication with nurses?
H1: Organizational ethical culture is positively related to patients’ rating of communication with nurses.
H01: Organizational ethical culture is not related to patients’ rating of communication with nurses.
RQ2: Is there a relationship between the dimension of clarity and patients’ rating of communication with nurses?
H2: Clarity is positively related to patients’ rating of communication with nurses.
H02: Clarity is not related to patients’ rating of communication with nurses.
RQ3: Is there is relationship between the dimension of congruency of supervisor and patients’ ratings of communication with nurses?
H3: Congruency of supervisor is positively related to patients’ rating of communication with nurses.
H03: Congruency of supervisor is not related to patients’ rating of communication with nurses.
RQ4: Is there a relationship between the dimension of congruency of management and patients’ rating of communication with nurses?
H4: Congruency of management is positively related to patients’ rating of communication with nurses.
Ho4: Congruency of management is not related to patients’ rating of communication with nurses.
RQ5: Is there a relationship between the dimension of feasibility and patients’ rating of communication with nurses?
H5: Feasibility is positively related to patients’ rating of communication with nurses
Ho5: Feasibility is not related to patients’ rating of communication with nurses
RQ6: Is there a relationship between the dimension of supportability and patients’ rating of communication with nurses?
H6: Supportability is positively related to patients’ rating of communication with nurses.
Ho6: Supportability is not related to patients’ rating of communication with nurses.
RQ7: Is there is a relationship between transparency and patients’ rating of communication with nurses?
H7: Transparency is positively related to patients’ rating of communication with nurses.
Ho7: Transparency is not related to patients’ rating of communication with nurses.
RQ8: Is there is a relationship between the dimension of discussability and patients’ rating of communication with nurses?
H8: Discussability is not related to patients’ rating of communication with nurses.
Ho8: Discussability is positively related to patients’ rating of communication with nurses.
RQ9: Is there is a relationship between the dimension of sanctionability and patients’ rating of communication with nurses?
H9: Sanctionability is positively related to patients’ rating of communication with nurses.
Ho9: Sanctionability is not related to patients’ rating of communication with nurses.
To measure the eight dimensions of the ethical culture of work groups, the questionnaire as developed by Kaptein (2008) will be used. The response to the 58 questions will be measured by using a 5-point Likert type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Riivari, Lämsä, Kujala and Heiskanen (2012) tested the eight variables of the CEV model. Cronbach’s α‘s were above 0.843, which suggests that all dimensions have relatively high internal consistency.
This study will analyze collected data to determine what relationship, if any, leadership ethical culture has with patient satisfaction. Correlational statistical techniques can show whether and how strongly pairs of variables are related. The main result of the correlation is the correlation coefficient (r). This measure ranges from – 1.0 to + 1.0. The closer it is to +1 and -1, the more closely the two variables are related either positively or negatively. However, when the value of r is close to 0, no relationship is found between the variables. Thus, correlational analysis will be used to determine the presence or absence of a significant relationship between the variables in the study. Meanwhile, descriptive statistics will be used to characterize the respondents and their answers to the individual survey items. A scatter plot between the mean of the ethical leadership dimensions and the mean of patient satisfaction scores, and a comparison of the mean of perceived ethical leadership for each of the eight leadership virtues will be performed.
The researcher will conduct assumption test before inferential statistical analysis. The assumption test is needed to ensure absence of significant outliers. In order to explore the relationship between the two variables, the researcher will upload the information into the SPSS 21.0 statistical software program to analyze results. The next step entails the researcher to conduct hypothetical tests as described above, and to conduct inferential statistics. Pearson product –moment correlation coefficients will be used to determine the relationship between the two variables. Pearson correlation will be used to determine if a statistically significant correlation exists between any of the eight CEV dimensions of leadership ethics and patient satisfaction rates. Pearson’s product-moment correlation coefficient (Pearson’s r) is a method to evaluate the linear relationship between two continuous variables. A relationship is linear when a change in one variable is associated with a proportional change in the other variable (Leech, Barrett, & Morgan, 2015). A Pearson correlation analysis will be the method to answer the research question related to the relationship between the eight CEV dimensions of leadership ethics and patient satisfaction related to nurses’ communication. In this case, the Pearson correlation determines the strength of the relationship between the ethical culture and patient satisfaction rates. With a multiple linear regression analysis, the researcher can use several independent variables to predict the dependent variable (Green & Salkind, 2013) by showing the degree of correlation between variables. Multiple regressions will be employed to determine the predictability of the criterion variables from the predictor variables.
The results will be presented through descriptive tables and figures. The researcher will check for alignment between the research questions, the research methodology, the instruments and variables. . Through a correlation design, the researcher will be able to perform data analysis in statistical procedure to test each hypothesis. Finally, the researcher will interpret the results and draw conclusions while discussing the implications of the study.
regression will be
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| DATA ANALYSIS PROCEDURES (Minimum one to three pages) | ||||
| Lists the problem statement or purpose statement, along with the research question(s). Also includes the null and alternative hypotheses for quantitative studies. | 2 | X | ||
| Describes in detail the relevant data collected for each stated research question and/or each variable within each hypothesis (if applicable). Quantitative Studies: “In detail” means scales (and subscales) of specified instruments AND type of data for each variable of interest. IMPORTANT: For (quasi) experimental studies, provide detailed description of all treatment materials per treatment condition, as part of the description of the independent variable corresponding to the experimental manipulation. | 2 | X | ||
| Describes, in detail, the data management practice including how the raw data were organized and prepared for analysis, i.e., ID matching of respondents who may respond to more than one survey/instrument, coding/recoding of variables, treatment of missing values, scoring, calculations, etc. Qualitative Studies: (1) describes transcription process for interviews, focus groups, descriptive statistics (mean scores, percentages) calculated for surveys, observation checklists, etc. | 2 | X | ||
| What: Describes, in detail, statistical and non-statistical analysis to be used and procedures used to conduct the data analysis. Quantitative Studies: (1) describe data file preparation (descriptive statistics used to check completeness and accuracy; for files from different sources, possibly aggregating data to obtain a common unit of analysis in all files, necessarily merging files (using the key variable defining the unit of analysis); (2) computation of statistics for the sample profile; (3) computation of (subscales and) scales; (4) reliability analysis for all scales and subscales; (5) computation of descriptive statistics for all variables of interest in the study (except those already presented in the sample profile); (6) state and justify all statistical procedures (“tests”) needed to generate the information to answer all research questions; and (7) state assumptions checks for all those statistical procedures (including the tests and / or charts to be computed). Qualitative Studies: This section begins by identifying and discussing the specific analysis approach or strategy, followed by a discussion of coding procedures used. Note: coding procedures may be different for Thematic Analysis, Narrative Analysis, Phenomenological Analysis, or Grounded Theory Analysis. | 2 | X | ||
| Why: Provides the justification for each of the (statistical and non-statistical) data analysis procedures used in the study. If a change in analysis was made, explains what was actually done versus what was planned and why. | 2 | X | ||
| How: Demonstrates how the statistical and non-statistical data analysis techniques align with the research questions/design. | 2 | X | ||
| Quantitative Analysis – states the level of statistical significance for each test as appropriate, and describes tests of assumptions for each statistical test. Qualitative Analysis – evidence of qualitative analysis approach, such as coding and theming process, must be completely described and included the analysis /interpretation process. Clear evidence from how codes moved to themes must be presented. | 2 | X | ||
| Provides evidence that quantity and quality of data is sufficient to answer the research questions. This must be present in this section or in an appendix including data samples. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Ethical Considerations
This quantitative study will follow the guidelines of the Institutional Review Board (IRB) of Grand Canyon University. Additionally, BRANY IRB approval from the Medical Center site will be sought prior to the data collection (Appendix B). Each of the participants will independently fill out an online survey without any outside influence. The researcher will assign a unique identification number to every participant to protect his or her identity, ensure confidentiality, encourage and maximize honesty of participant rating. Nurses and patient participants will complete the survey on a voluntary basis and can withdraw at any time.
Prior to the beginning of the study, each participant will be informed of the purpose of the research and the benefits of participating. Furthermore, participation will be voluntary with informed consent explaining the purpose of the research and how the privacy and identity of the participant will be protected. An informed consent statement will be obtained from each participant prior to responding to the surveys. An informed consent form will include the name of the investigator, contact information, purpose of the study, risk and benefits, data collection and storage. Filling out the online survey is considered consent to participate, as indicated in the cover letter. The author is a member of the research site. In conducting this research, the author is aware of his dual role as both a researcher and organizational leader. Therefore, he will set out a recruitment process that allows voluntary participation in the research. Participation will be voluntary and would be treated with confidentiality and all participants will anonymously be identified by a code to ensure confidentiality. The researcher will not give any monetary reward for participation in the study.
Through Survey Monkey®, the researcher will send invitation letters and consent letters to potential participants who have agreed online to gain access to the link for the survey and questionnaire. The OpinionMeter will be administered to the patients by the hospital hospitality representative. The questionnaire is in English. However, for non-English speaking participants, the representative will be able to use a translation phone to communicate with these patients. The researcher will treat all participants as anonymous agents and provide each individual with unique access to the questionnaire and survey on Survey Monkey®. In order to assure the confidentiality of participants, surveys and questionnaire for this research will not contain identifying information such as mail addresses. Additionally, unbiassed language will be used. The participants may choose to withdraw from participating in the study at any time. All data and files gathered during the research study will be secured in a locked filing cabinet. The participants will not receive any kind of reward or compensation for their participation in the study. The data will be maintained for five years, after which the data will be destroyed.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| ETHICAL CONSIDERATIONS (Minimum three to four paragraphs or approximately one page) | ||||
| Provides a discussion of ethical issues, per Belmont Report and IRB guidelines, related to the study and the study population of interest. Explains which principles / issues are relevant to the study. Identifies the potential risks for harm that are inherent in the study. | 2 | X | ||
| Describes the procedures for obtaining informed consent and for protecting the rights and well-being of the study sample participants. | 2 | X | ||
| Addresses key ethical criteria of anonymity, confidentiality, privacy, strategies to prevent coercion, and any potential conflict of interest. | 2 | X | ||
| Describes the data management procedures adopted to store and maintain paper and electronic data securely, including the length of time data will be kept, where it will be kept, and how it will be destroyed. Explains what he/she planned to do / did to implement each of the principles / issues that are relevant the study data management, data analysis, and publication of findings. Note: Learners are required to securely maintain and have access to raw data/records for a minimum of three years. If asked by AQR reviewer or CDS representative, learner must provide all evidence of data including source data, Excel files, interview transcripts, evidence of coding or data analysis, or survey results, etc. No dissertation will be allowed to move forward in the review process if data are not produced upon request. | 2 | X | ||
| Includes copy of IRB Informed Consent (Proposal) and IRB Approval letter (Dissertation) in an Appendix. All approvals, consent forms, recruitment, and data collection materials are mentioned in the Data Collection section and included in separate appendixes (with appropriate in-text references). | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. | ||||
| Reviewer Comments: |
Limitations and Delimitations
The generalization value of the data produced by the study is limited. The results cannot be generalized to the other educational institutions or studies. The study will take place in a singular healthcare organization in New York City with differences in geography, culture and social economic status compared to other healthcare organizations. Several limitations are inherent to the research method adopted for this study. First, the research methodology will be limited to a quantitative approach and will not involve a qualitative portion which limits the insight of the work environment among the medical surgical nurses. The survey response will be limited to one-time data period in 2018. The correlational design of the study can be seen as a limitation. The findings of the study will mainly provide knowledge about medical and surgical units and will pose limitations to generalizability to other organizations in different geographical location.
The OpinionMeter survey selected for the study could also be viewed as a limitation of the study. The limitations of the OpinionMeter is the language in which the survey is available, as it is only available in English. However, the independent surveyor will assist patient by using a translation phone. Another limitation of the OpinonMeter is that it is based on the HCAHPS measurement and might only indicate one organizational outcome. HCAHPS instrument might not play a significant role in the formation of overall hospital quality improvement (Westbrook, Babaku, & Grant, 2014). However, there are many important quality indicators of patient care, such as patient injury which can affect patient satisfaction. This research will be limited to patient satisfaction related to nurses’ communication, therefore, the researcher suggested further studies to explore the relationship between ethical culture and other organizational outcomes such as patient injury and hospital-acquired infection.
Delimitations of the research include the chosen participants of the study, as each participant was a registered nurse with at least one-year experience. The research only took into account the perspective of a specific group of frontline employees who are registered nurses. The study only accounts for the viewpoint of a registered nurse that holds no leadership position within the healthcare organization. Other frontline staffs, such as support staffs, were not included. Furthermore, leaders, such as nursing managers and supervisors, were excluded from the study. Another delimitation centers on the fact that the study is intentionally confined to Kaptein’s (2008) model of corporate ethical virtues and one item from the HCAHPS survey which relates to nursing communication with patients. There may be other ethical leadership attributes not mentioned or examined in this study that could have contributed to patient satisfaction. The researcher focused on the two main inpatient units which are the main indicators of the hospital’s patient satisfaction scores, and purposefully not eliminating units based upon status of performance and size. To minimize and/or mitigate negative consequences of limitations and delimitations, the researcher will employ careful procedures to ensure all the 128 participants involved in the study will be properly informed and will receive all of the necessary information in a timely manner.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| LIMITATIONS AND DELIMITATIONS (Minimum two to three paragraphs) | ||||
| Reiterates those limitations listed in Ch. 1 and explains why the existing limitations are unavoidable. Describes any delimitations related to the methodology, sample, instrumentation, data collection process and analysis. Note: This section must be updated as limitations emerge in the data collection/analysis, and then incorporated in Chapter 5 the limitations overall and how the study results were affected. | 2 | X | ||
| States consequences of each limitation and delimitation in terms of data quantity, quality, and validity / generalizability of the findings. Discusses strategies to minimize and/or mitigate the negative consequences of limitations and delimitations. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. |
Summary
The issue of organization’s ethics is a global problem. The challenges facing healthcare requires strong leadership. The healthcare industry is unique because it depends upon human beings caring for one another. Thus, patient care is dependent on healthcare professionals. Therefore, it is importance to align and promote ethical working environment. When healthcare organization possess high level of ethical culture, they experience less staff turnovers, more productivity, better level of patient safety, cost saving and high level of patient satisfaction (Cohen, Foglia, Kwong, Pearlman, & Fox, 2015). Therefore, improving employees’ perceptions of ethics in the organization could have impact on healthcare organizational outcome.
Studies have shown a relationship between ethical culture and organizational outcomes (Yidong & Xinxin, 2013; Neubert, Wu, & Roberts, 2013; Schaubroeck et al., 2012; Kacmar, Carlson, & Harris, 2013; Neubert, Wu, & Roberts, 2013; Demirtas & Akdogan, 2013; Sharif & Scandura, 2014; Neves & Story, 2015; Kaptien, 2011, 2016). The topic of ethical culture plays a critical role in organizational innovation and subsequent, sustainable performance (Riivari & Lasma, 2013). One limitation of this study is that the researchers are unable to study other groups of outcomes, namely employee and financial consequences.
Several researchers examined leadership ethics effects on job performance. However, leadership ethical virtues and the relationship to patient satisfaction as a result of nursing communication have not been explored. The need to identify and examine frontline nursing employees’ perceptions of leadership ethical culture is imperative. This knowledge could have practical implications for organizational performance and patient satisfaction. The implication of effective patient communication can potentially lead to increased patient satisfaction. Improved nurse-patient communication would improve quality care, potentially decrease in anxiety, foster safety, and enable patients to develop trust in nursing care, which has the opportunity to lead to increase patient satisfaction (Oni, 2012).
The purpose of this quantitative correlational study is to explore whether or not the relationship between nursing ethical virtues, as perceived by frontline nursing staff, is significantly related to patient satisfaction related to nurses ‘communication at a healthcare organization in New York City. A quantitative approach is selected to test the null hypothesis. Following Institutiona Review Board’s (IRB) approval to collect data and site authorization from the organization, the data will be collected in one healthcare organization. The total target employees of this study are 200 frontline nursing staff from inpatient medical surgical registered nurses (RNs).
Data collection for this quantitative correlational study will be administered to a sample size of 128 RNs through electronic administration of the CEV questionnaires and the OpinionMeter will be administered to patient that were assigned to the same nurse. The eight dimensions of the CEV model (Kaptein, 2008) will serve as the independent variable. The patient satisfaction related to nurses’ communication will be administered through the OpinionMeter which is based on the HCAHPS measurement and will serve as the dependent variable.
The CEV questionnaire will be administered online and analyzed using the SPSS statistical software package. A Pearson correlation will be used to determine if a statistically significant correlation exists between any of the eight CEV dimensions of leadership ethics and patient satisfaction. Ethical consideration and protocol, especially beneficence, respect for persons, and justice as outlined in the Belmont Report (1979) and Grand Canyon University’s Institutional Review Board (IRB) will be strictly observed and implemented throughout the study process.
In this study, the researcher will attempt to investigate nursing ethical virtues and attributes to organizational outcomes of patient satisfaction. Research related to the relationship of nursing ethics to other organizational outcomes continues to expand, and the need for further research in the area of nursing ethical leadership may require other frontline healthcare employees such as support staff, and mid-level managers to participate. Nursing leaders will continue to be challenged to find the best styles of leadership that suit and address patient satisfaction and organizational outcome. Healthcare leaders need to clearly understand the organizational influences (particularly leadership ethical virtues) that may affect patient satisfaction. The findings of this study could provide recommendation for teaching, strategic planning and change in order to improve patient experience. Chapter 4 will present the result of the data analysis and discussion of the findings.
| Criterion *(Score = 0, 1, 2, or 3) | Learner Score | Chair Score | Methodologist Score | Content Expert Score |
| LIMITATIONS AND DELIMITATIONS (Minimum two to three paragraphs) | ||||
| Reiterates those limitations listed in Ch. 1 and explains why the existing limitations are unavoidable. Describes any delimitations related to the methodology, sample, instrumentation, data collection process and analysis. Note: This section must be updated as limitations emerge in the data collection/analysis, and then incorporated in Chapter 5 the limitations overall and how the study results were affected. | 2 | X | ||
| States consequences of each limitation and delimitation in terms of data quantity, quality, and validity / generalizability of the findings. Discusses strategies to minimize and/or mitigate the negative consequences of limitations and delimitations. | 2 | X | ||
| Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format. | 2 | X | ||
| *Score each requirement listed in the criteria table using the following scale: 0 = Item Not Present or Unacceptable. Substantial Revisions are Required. 1 = Item is Present. Does Not Meet Expectations. Revisions are Required. 2 = Item is Acceptable. Meets Expectations. Some Revisions May be Suggested or Required. 3 = Item Exceeds Expectations. No Revisions are Required. |
Students working on case studies or might need academic help, might find our custom Case Studies Writing Services helpful.
Also look at some of our business services
– Business Essay Writing Service
– Business Dissertation Writing Services
– Business Report Writing
– Business Assignment Help
– Business Planning Writing Service
– Business Assignment Writing Service
Here you can check some of our dissertation services:
– Dissertation Writing Services
– Write My Dissertation
– Buy Dissertation Online
– Dissertation Editing Services
– Custom Dissertation Writing Help Service
– Dissertation Proposal Services
– Dissertation Literature Review Writing
– Dissertation Consultation Services
– Dissertation Survey Help
Here are some the nursing writing services we provide:
– Nursing Dissertation Writing Services
– Nursing Paper Writing Services
– Nursing Essay Writing Service
– Nursing Assignment Help