



The influence of the Ethnicity and Cultural Background in the delay for Screening Colonoscopy in Hispanic Males over the age of fifty
Abstract
Study background: Cancer of colorectal is one of the ordinarily diagnosed diseases and the second prime cause of death in the United States. However, early diagnosis and treatment can decrease CRC-related horribleness and mortality. Nearly 66% of patients are diagnosed with advanced malady showing non-adherence to prescribed screening guidelines. Indeed, not as much as half of people more than 50 years old get screened at suggested intervals. Hispanics constitute the biggest ethnic/racial class in the United States representing 17.4% (55.4million/318 million) of the aggregate US populace in 2014 (CA Cancer J Clin 2015). Lower level of Hispanic people are screened for colorectal cancer when contrasted to Blacks and Whites. The absence of learning and the negative observations about the colonoscopy system may compel a low consistency for colorectal screening among Hispanic people. The absence of information and the negative discernments about the colonoscopy system may compel a low consistency for colorectal screening among Hispanic people. Screening limit including “machismo,” misperceptions, shame, and humiliation. Apprehension toward expanding screening of colorectal cancer will be helpful among Hispanics. Training, increment doctor guiding and referral, may diminish stigma and different boundaries, by expanding the learning in the Hispanic people group toward colorectal malignancy screening.
Purpose: The main purpose of this research was to comprehend the retard screening for colorectal cancer among Hispanic men of age fifty years and above.
Method: The method employed for this research was qualitative research. Hispanic males were interviewed under the time frame provided by the “The American College of Gastroenterology.”
Introduction
This research was about the impact of the Ethnicity and Cultural Background in the retardation for Screening Colonoscopy in Hispanic Males beyond fifty years old. The purpose of the study was to understand the retard for colorectal cancer screening among the Hispanic men who were 50 years and above. Qualitative research method was used in the study. Ten Hispanic men were interviewed who decided to do colonoscopy screening as provided by the by “The American College of Gastroenterology.” As indicated by “Journal of the National Comprehensive Cancer Network,” colorectal cancer (CRC) is the fourth most as often as possible diagnosed a tumor and the second driving reason for cancer disease death in the United States. In 2013, roughly 102,480 new instances of colon tumor and around 40,340 instances of rectal cancer tuned out. Amid that year, 50,830 individuals died of colon and rectal malignancies consolidated. Cuban, Mexican, Puerto Rican, Central or South American, Dominican, or other Spanish plummet are the second biggest racial/ethnic gathering in the United States after non-Hispanic whites (NHWs). The US Census Bureau appraises that 55.4 million Hispanics were living in the United States in 2014, containing 17.4% of the aggregate populace.
Particularly, existence of lower rates CRC screening rates are among the class of those recognized as being of Hispanic root, the uninsured, disabled people, and women. In a 2011 report from the National Center on Health Statistics apprehending the effect of financial status (SES) on the well-being of the country, just 47% of Hispanic respondents announced any colorectal disease screening method (2010). This is in contrast with 59% of all grown-ups, ages 50 – 75 years, paying little heed to race. Evidence proposes that screening for CRC can diminish CRC death rates.
The malicious form of CRC blossoms from a considerate polyp that can be detected through screening methods. The essential screening techniques for CRC incorporate the fecal occult blood test (FOBT), colonoscopy, sigmoidoscopy and the prescribed screening interims for each incorporate one year, five years, and ten years, respectively. Despite the solid proof supporting the advantages of CRC screening and bringing about the decrease in mortality, low rates of screening among in endangered people will bring about an anticipated 50,830 demises from the infection this year.
With such tremendous obligation caused by a conceivably preventable malady, the U.S Department of Health and Human Services (DHHS) has set up objectives and targets to build CRC screening by means of its initiative of Healthy People 2020. From 2008 to 2010, DHHS revealed an expansion in CRC screenings from 52.1 to 59.1 percent. By 2020, DHHS expects to expand screening to a rate of 70.5 percent.
To enhance CRC screening rates, particularly among places where screening rates are lower, we have to build our comprehension of what factors impact screening among these populations. DHHS noticed that the weight of CRC ailment is disseminated unequally among poor, ethnic and racial minorities given numerous components, including dialect or social contrasts with human services suppliers. This dialect obstruction, known as Limited English capability (LEP), has been recorded in writing as a hindrance to CRC screening among varying subgroups of Spanish speaking Latinos. For instance, in an investigation dissecting information from the Medical Expenditure Board Survey (MEPS) focused on comprehending patient-supplier correspondence and dialect obstructions affecting CRC screening. Those patients who did not speak English experienced not as much as a large portion of the probability of being screened for CRC than did the patients who spoke English.
This screening test is requested to recognize infection at a beginning time for asymptomatic patients, on the other hand, demonstrative tests are requested for patients with s/s of sickness. Colorectal screening tests incorporate fecal immunochemical test (FIT), twofold differentiation barium douche, fecal mysterious blood test (FOBT), Colonoscopy and adaptable sigmoidoscopy.
As per “The Rules of the American College of Gastroenterology,” the particular rules for colorectal malignancy screening are as per the following:
- Tests that forestall malignancy are favored over those that solely recognize growth.
- The favored colorectal growth anticipation test is colonoscopy utmost ten years, starting at age 50 years, however, in African Americans, it is 45 years of age.
- For patients who spurn colonoscopy or another tumor anticipation test, the desired cancer diagnose test is FIT, administered yearly.
Auxiliary cancer diagnosis tests prescribed in the ACG criterion are as per the following:
- Flexible sigmoidoscopy every 5-10 years.
- CT colonography utmost five years, which substitutes two-fold difference barium bowel purge as the radiographic screening elective for patients who repudiate colonoscopy.
Surrogate growth diagnosis tests in the ACG rules are as per the following:
- Fecal DNA testing utmost three
- Annual Hemoccult Sensa.
For purposes of screening, patients with one first-degree relative determined to have colorectal tumor or propelled adenoma at age 60 age or more established are considered at normal hazard. For patients with a solitary first-degree relative are determined to have colorectal malignancy or propelled adenoma before the age 60 years. Those with two first-degree relatives with colorectal growth or propelled adenomas, the procedure suggests colonoscopy utmost five years. Starting at age 40 years or ten years.
The study assisted in addressing the misperception of Hispanic male toward the screening of colorectal cancer and the hazard that causes the deferral. This study also contributed to comprehend the result, assuming any, after the screening test was finished.
Problem statement
What is the impact of the Ethnicity and Cultural Background in the delay for Screening Colonoscopy in Hispanic Males beyond fifty years old? The analysis addressed the misperception of Hispanic guys toward colorectal disease screening and the peril that caused the retardation. The study helped to comprehend the consequences that could have occurred after the screening test. The main objective of the study was to educate the people of the consequences that could arise in case preventable measures were delayed. In my seven years of being a Gastrointestinal Nurse, I was aware of the possible consequences for delayed screening of colorectal cancer. I saw that colorectal cancer that can be treated with a positive prognosis. I also saw that colorectal cancer has the sole therapy of palliative care. Additionally, I have come across patients of 70 years of age that have not undergone screening of colorectal cancer without any repercussions.
The study concurred with other researches about the misperception of colorectal cancer screening. U.S. Hispanics are at more serious hazard for prior beginning and have brought down age-balanced survival rates for CRC than their non-Hispanic White partners. (Jemal, Siegel, Xu, and Ward, 2010). As indicated by “National Center for Biotechnology Information, U.S. National Library of Medicine,” The U.S. Hispanic populace, specifically, reflects low rates of CRC screening. Keeping in mind the end goal was to get an extensive comprehension of obstructions to CRC screening in this populace. An integrative audit was performed in PubMed and CINAHL from 2002 to 2018, and eight examinations on different boundaries to CRC screening among the U.S. Hispanic populace were inspected. Discoveries perceived dread, cost, and absence of mindfulness as normal obstructions to CRC screening and more particular hindrances material to the Hispanic populace being low proficiency/instructive levels and absence of supplier suggestions. The research demonstrated socially particular obstructions to CRC screening among Hispanics, the biggest being constrained English aptitude. The audit exhibited a requirement for extra focus on approaches, education awareness, and guidance of the provider as approaches to enhance CRC screening in Hispanics.
As a family nurse practitioner, we have sovereignty to assume responsibility and liability for wellbeing advancement and support, diagnosis, patient issues, and evaluation. We can instruct the Hispanic male group about the misperception of colorectal tumor screening. We can teach what a colonoscopy is and the method prior and then afterward. We can instruct about the Guidelines for preventive measure. We can work together to expand doctor recommendation and referral. At last, we can educate the society about the diverse assets in the event that they are in need a colorectal disease screening.
Literature review
Colorectal cancer
Rectal and colonic cancer is referred to as colorectal cancer (Iversen, 2012). It is characterized by malignant growth which take place in the large bowel which is locally confined before metastasis via the bowel wall to the lymph nodes and other body parts (Potter, 1995; Campbell, 1999). Cancer of the colon varies from the caecum to the sigmoid and rectal cancer starting from the recto-sigmoid to the anus (de Heer, 2007).
Epidemiology of colorectal cancer screening
Colorectal cancer is ranked third on the commonly diagnosed cancer in the world with 1.23 million incidence of new cases per year (Ferlay et al., 2010). Colorectal cancer screening is widespread in the Western World with the aim of reducing colorectal cancer mortality and incidence. Colorectal cancer is among the third commonly diagnosed cancer and ranked second leading cause of deaths caused by cancer in the United States (Percac-Lima et al., 2008). Less than half Hispanic individuals above the age of 50 years get screened at intervals that are recommended (“Colorectal Cancer”, 2018). Diverse researches have been promulgated in regards to the misinterpretation of the colonoscopy in the Hispanic male populace. The European Union recommended the screening of colorectal cancer in 2010 (Segnan et al. 2010). As indicated by “American Association for Cancer Research,” colorectal malignancy (CRC) causes 27% of all tumor deaths among Puerto Rican Hispanics (PRH). The incidence of colorectal cancer is higher in developing countries which result to over a third of new cases of CRC to the annual worldwide incidence (GLOBOCAN, 2008).
Aetiology and risk factors
Aetiology of colorectal cancer is complex and include interaction between inherited susceptibility and environmental factors (Wallin, 2011). Colorectal cancer occurs in two common forms: inherited colorectal cancer and sporadic colorectal cancer. Most CRC cases are because of sporadic hereditary or epigenetic occasions that prompt the improvement of the tumor (Kang et al., 2011). In sporadic cases, genetic variations take place which are caused by etiologic factors for instance lifestyle factors, age and environmental factors.
Age
CRC disease risk increases with age although it affects all ages. The age related exponential rises in the incidence of CRC by accumulation of genetic events in the tissues that are ageing (DePinho, 2000). After someone attains the age of 40 years, the probability of being diagnosed with CRC rises especially at the age of 50 years which increases sharply (Food, 2007; Ries et al., 2008). The rate of incidence is over 50 times higher in individuals aged 60 to 79 years than those individuals who are below the age of 40 years (Society, 2005; Ries at al., 2008). In the United States, colorectal cancer currently is one of the 10 most commonly diagnosed cancers among women and men aged 20 to 49 years (Fairley et al., 2006).
Behavioral and lifestyle factors for colorectal cancer
Diet has been studied as one of the possible risk factors over the years. Terry et al., (2001), depicted a relationship between low vegetable and fruit intake and increased colorectal cancer risk. It is hypothesized that fibre, folic acid, antioxidant vitamin, phytochemical and micronutrient content in fruits and vegetables may have a protective effect against CRC. Some observational studies noted an inverse association between dietary fibre consumption and the risk of CRC (Negri et al., 1998; Lin, 2009). Cooked meat at high temperatures leads to production of aromatic hydrocarbons and heterocyclic amines which is believed to have carcinogenic properties that cause cancer (Sinha, 2002; Santarelli et al, 2008).
Exercise role in reducing the risk of colorectal cancer has been well established (Fung & Brown, 2013). A meta-analysis that took place in 2009, concluded that regular exercise lowered the risk cancer of the colon by almost 25% in both women and men (Wolin et al., 2007). Exercise help to lower levels of prostaglandins decreasing gut transit time and improving immune function (Samad et al., 2005). Individuals with BMI more than 30Kg/m2 have a 20% greater risk of CRC development as compared to normal weight controls (Moghaddam et al., 2007).
Elevated blood sugar, hypertension, Type-2 diabetes and hyperinsulinemia are metabolllic abnormalities linked with the syndrome of insulin resistance that also independently relate with colorectal cancer (Giovannucci, 2007). Type-2 diabetes increses the risk of colon cancer by 30% (Larsson et al., 2005).
Environmental factors and lifestyle
Migrates and their offspring studies provides evidence on risk of the environment to CRC. Rates of incidence on CRC tends to rise among migrants from low-risk to high risk countries (Janout & Kollarova, 2001). Urban residents have a higher incidence of colorectal cancer with higher incidence rate among men than women (Boyle & Langman, 2000).
Non-sporadic colorectal cancer
Inherited CRC accounts for 5% to 10% in all colorectal cancer cases. Some families to germ line mutations in specific genes (Cherry, 2011).These episodes sum up to cause CRC carcinogenesis and include genes that direct cell development and separation. The common genetic syndromes are familial adenomatous polyposis (FAP) syndrome and hereditary non polyposis colorectal cancer (HNPCC) syndrome (Segelman, 2012). Conditions and syndrome that are less common include Turcot’s syndrome, Gardener’s syndrome, oldfield’s syndrome, juvenile polyposis, Peutz-Jeghers disease and Cowden disease (Scott, 2003). Enhancing comprehension of the molecular episodes that prompt CRC carcinogenesis can diminish CRC mortality by risk stratifying individuals and in addition creating aversion techniques. CRC risk in patients with ulcerative colitis is related to the duration of symptoms and estimated at 2% after a duration of 10 years, 8% after 20 years and after 30 years it is 18% (Eaden et al., 2001).
Additionally, as per “US National Library of Medicine National Institutes of Health,” national colorectal malignancy (CRC) rate rates have consistently diminished, the rate for Hispanics has been expanding and screening rates are low. Machismo developed as a greater amount of impact for Hispanics, who communicated worry over colonoscopies being possibly transformative and trashing. This examination features the significance of recognizing diverse attributes to comprehend screening hindrances better and give ideal CRC screening directing in essential care settings. A scope of framework, supplier, and patient obstructions for Hispanics across the nation have been reported in past investigations went for understanding hindrances to CRC screening in essential care (Walsh & McPhee, 1992). Patients’ convictions and dispositions incredibly impact their CRC basic leadership forms and are hence an essential locus for potential intercessions to enhance screening consistency (Jandorf et al., 2009).
One cultural component that influence the screening of CRC among Mexican men is machismo (Getrich et al., 2012). Evolving amid the nineteenth century after Latin American nations attested their freedom from earlier Spanish manage, machismo was at first framed as an idea that characterized male predominance over ladies and can be portrayed as the dispositions and characters related with manhood seen among Hispanic men (Mayo & Resnick, 1996). This social factor is as yet common among Hispanic men today and has been recorded as a specific obstruction to look for safeguarding medicinal services measures (Getrich et al., 2012).
Machismo has been described as an arrangement of identities and attitudes related with masculinity (Sobralske, 2006). The term has been speculated in various routes by journalists, therapists, students of history, sociologists, anthropologists, and pundits in the famous media (Arciniega, Anderson, Tovar-Blank & Tracey, 2008; Neff, 2001). There is a concession to the indication of machismo and the associated descriptors macho and machista, which mark men who show machismo; indeed, the terms have been characterized as having various and fluctuating implications (Guttman, 1996). In spite of the fact that it regularly transmits an undertone of being a common laborer and rustic peculiarity, the idea of machismo has been utilized to characterize men from a grouping of class encounters and geographic districts (Guttman, 1996). The objective is far reaching all through Latin America and among U.S. Hispanic places. In the U.S. setting, Machismo has conveyed both bigot and patriot suggestions when used to depict both outside and U.S (Guttman, 1996).
The research tended to the misperception of Hispanic men toward colorectal malignancy screening and the danger that leads to the postponement. The hypothesis utilized was Health Belief Theory (HBM). The model places that an individual will embrace a preventive well-being measure if the individual trusts the condition to be kept away from is not important. He or she is vulnerable to the condition, the intercession suggested will keep the condition, and there are no staggering boundaries to receiving the medication (Rosenstock, 1974; Rowley, Loader, Sutera, Walden, & Kozyra, 1991).The utilization of the HBM has been compelling in surveying and inspiring wellbeing conduct change among African Americans with respect to tumor screening, hereditary data, and diabetic social insurance consistence (Gustafson, Gettig, Watt-Morse & Krishnamurti, 2007).
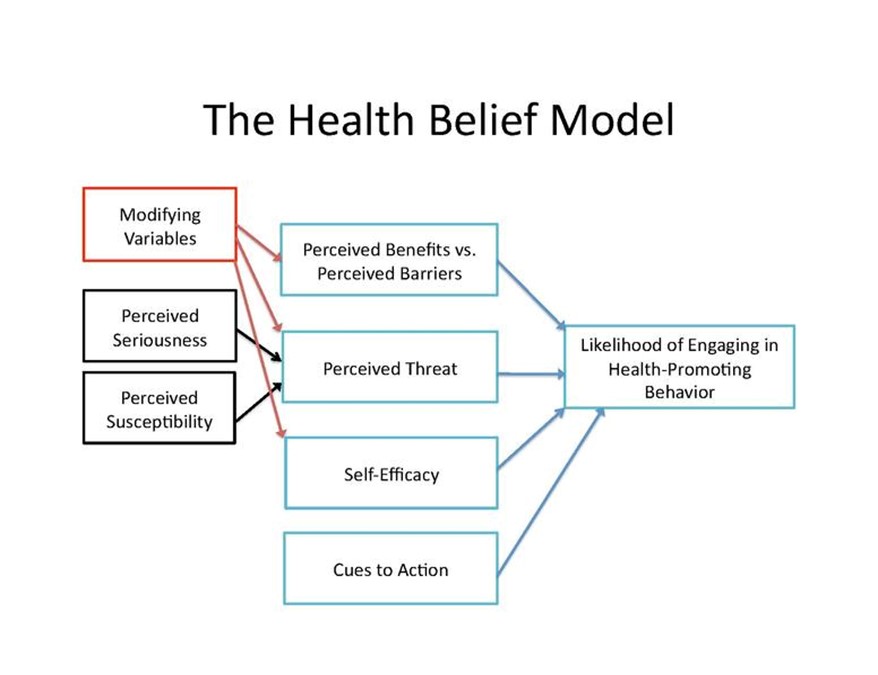
Figure 1 the Health Belief Model
Methodology
The study was about descriptive and qualitative research in which a questionnaire was used to collect data from the participants. The members were approximate of ten asymptomatic Hispanic males more than 50 years of age that never had a colonoscopy that chose to do the Colorectal malignancy screening test to identify ailment yet was at that point over the time span of safeguard measures. They were given a questionnaire with four inquiries:
- In your own words depict what a colonoscopy method is?
- Perception of a colonoscopy?
- What prompts you to have a colonoscopy now?
- What do you anticipate from the Colonoscopy?
The study was carried out at Kissimmee Endoscopy Center, an outpatient surgical focus. The standard patient workload was around 40 systems for each day, and the greater part of the patients were Hispanic/Latinos. Approval was requested from the Center for the Study. The patient interview took around 20 minutes and was done in the pre-agent zone. Ten Hispanic guys were interviewed for the investigation. They were given the composition assent toward the start of the confirmation procedure. At that point, later the poll was directed amid the Pre-operation process. The instruments that were utilized are Microsoft Word to transcript the meeting. Atlas-ti 7.0 software was utilized for the investigation of the data. The research helped established researchers by investigating the explanations behind the absence of consistency with the colonoscopy system in the Hispanic guys. This study helped other people to comprehend the significance of following the procedures from “The American College of Gastroenterology” for impediment. The investigation additionally helped in creating understanding among Hispanic guys to have a divergent impression toward the colorectal malignancy screening.
For this specific examination, appraisal of data identification with CRC screening practices among men reacting as being of Hispanic or Latino ethnicity ages 50 and more seasoned was be incorporated. As indicated by the U.S 2010 Census, “Hispanic or Latino” alludes to a man of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or inception paying little respect to race. Related to ethnicity, respondents were asked the questions, “Are you Hispanic or Latino?” The accompanying reaction choices were incorporated: yes, no, don’t have the foggiest idea/not certain, or refusal. For ages, respondents were asked the question, “What is your age?” The accompanying reaction alternatives incorporated the following: do not have the no idea/not certain, rejected, age 18-24, age 25-34, age 35-44, age 45-54, age 55-64, and age 65 or more established. For this specific investigation, age was dichotomized into two: 49 years below and above 50 years; just the last group was examined.
Drawn from the BRFSS, information included overview reactions from people living in family units over the 50 United States, the District of Columbia, Guam, and Puerto Rico. Information gathered from Hispanic men living in Puerto Rico, involving very nearly 54% of the first example of men showing Marianismo, were prohibited from this investigation because of different variables. The purpose of this investigation was to inspect the impact of ethnicity and cultural background in the postponement of Screening Colonoscopy in Hispanic Males beyond fifty years old. Hispanics living in Puerto Rico encounter diverse ways of life, conditions, and access to human services contrasted with Hispanics from Puerto Rico living on the terrain of United States. With respect to human services access, in 1993 Puerto Rico embraced another social insurance change, known as “the Reforma.”
The Reforma privatized medical services to lessen the increasing expenses troubling the Puerto Rican government and increments to bring down expenses. It also enhanced the wellbeing results for Puerto Ricans who were already secured under Medicaid and Medicare and whose livelihoods were underneath 200% of the neediness level. Although the U.S social insurance framework imparts a few attributes to the Puerto Rican human services framework, numerous distinctions affect people’s access to use the framework. For instance, in a cross-sectional examination inspecting contrasts in the Medicare encounters of recipients in Puerto Rico contrasted and those in the U.S, specialists found that recipients in Puerto Rico detailed more negative encounters than U.S recipients for getting required care, receiving the required care rapidly, and vaccination. Scientists credited the discoveries to the lower subsidizing of medical care services benefits in Puerto Rico in respect to the U.S. Additionally, Hispanic men living on the territory might encounter cultural assimilation, not at all like the Hispanic men living in Puerto Rico. Cultural assimilation can be characterized as “changes that happen after some time when two societies come in persistent contact.”
Variables
Independent variable
Two independent variable, ethnicity and cultural background were constructed from the sample to analyze the impact of cultural background and ethnicity on the delay of colonoscopy screening of Hispanic male above the age of 50 years and above. They were built from the accompanying statistic factors; conjugal status, work status, and essential dialect communicated in. Members were given the following reaction alternatives: married, separated, widowed, isolated, never married, an individual from an unmarried couple, or refused. For work status, members were given the following reaction choices: utilized for compensation, independently employed, out of work for over one year, out of work for under one year, a homemaker, an understudy, resigned, unfit to work, or can’t. For primary dialect spoken, members were given the following reaction choices: English, Spanish, or other. Every one of the factors was dichotomized, and after that, the independent factors were developed for examination.
Validity and reliability
Validity
Validity refers to the degree to which research instrument measures what it purports to measure (Mugenda, 2003). According to Orodho (2004) validity in a sense raised, is the degree to which the empirical measure of the concept, accurately measure the concept. To validate the questionnaire, a pilot survey was carried out to the selected separate respondents, but a similar sample to the one in the study.
Reliability
The reliability of research instrument conserves the extent to which the tool yields the same results on repeated trials hence, the tendency towards consistency found in repeated measurements in what is referred to as the reliability of the of the research instrument. In this study reliability followed the following steps, the developed questionnaire was given to a few identical respondents subjects not included in the main study the answered questionnaire was answered manually. After two weeks the same questionnaire was administered to the same group of subjects.Thus, test-retest method was used, the consistency in the answers assured reliability of the instrument.
Research Ethics Committee of the Nursing Department of the University of Ana G Méndez requested the consent which followed the procedure to protect the rights of humans following the criteria established by the IRB. The IRB guidelines are as follows:
- Risks to subjects are minimized by using procedures which are consistent with sound research design and which do not unnecessarily expose subjects to risk.
- Selection of subjects is equitable.
- Informed consent will be sought from each prospective subject or the subject’s legally authorized representative, by, and to the extent required by46.116.
- When appropriate, the research plan makes adequate provision for monitoring the data collected to ensure the safety of subjects.
- When appropriate, there are adequate provisions to protect the privacy of subjects and to maintain the confidentiality of data.
- All records will be stored safely inside a locked cabinet for six
Findings of the study
Statistical analysis
To examine whether colonoscopy screening was affected by cultural background and ethnicity, descriptive analyses were initially performed, looking at the proportion of each group reporting screening or not. Next, using each of the dichotomized HBM construct or construct components as outcomes, seventeen logistic regressions with robust standard errors were performed to test potential associations with race/ ethnicity and cultural background. All adjusted cultural background. Models included covariates measuring health access, demographic characteristics, health status, and physician recommendation of screening. Wald tests were used for establishing associations between ethnicity and cultural background with colposcopy screening.
The participants who participated in the study and were Hispanics. Baseline information shows that 10 Hispanic men ages 50 who participated in the study had not undergone the colonoscopy screening. It shows that cultural background and ethnicity affected the screening of colonoscopy. 70 % of the participants had undergone colonoscopy screening while 30% had not done the screening according to table 1.
Table 1 colonoscopy screening of Hispanics men above the age of 50 years.
| CRC screening | Ethnicity (n=5) | Cultural background (n=5) |
| n (%) | n (%) | |
| Any CRC test | ||
| Never received Any Test | 30 | 70 |
| Not up to date on any test | 35 | 65 |
According to a research conducted by Thompson (2014) on how Marianismo affected the screening of colonoscopy screening of women it showed that culture had the same effect on the screening of colonoscopy. From his data of 7,101 women aged 50 years and older, Marianismo which is cultural aspect affecting both women and men from the Hispanic origin as depicted by the following results in table 2.
Table 2 Crude Odds of CRC screening behaviors among Hispanic women ages 50 and older exhibiting Marianismo characteristics (n=7,101)
| CRC screening behaviors | Marianismo
(n=355) |
Non-Marianismo
(n=6,746) |
||
| N (%) | OR (95%CI) | P-Value | N (%) | |
| Any CRC Test | ||||
| Never Received Any Test | 169 (49.7) | 2.05 (1.647,2.554) | .000* | 2,005 (32.5) |
| Not Up to Date on Any Test | 170 (55.0) | 2.077 (1.650,2.616) | .000* | 2,083 (37.1) |
| FOBT | ||||
| Never Received FOBT | 280 (82.1) | 1.633 (1.231, 2.162) | .001* | 4,450 (73.8) |
| Did Not Receive FOBT in the past year |
30 (49.2) | 0.554 (0.332, 0.924) | .002* | 1,029 (63.6) |
| Sigmoidoscopy/Colonoscopy | ||||
| Never Received Sig./Col | 199 (58.7) | 2.207 (1.767, 2.756) | .001* | 2,415 (39.2) |
| Did Not Receive Sig. in the past 5 years | 2(16.7) | 0.397 (0.085, 1.861) | .226 | 73 (33.5) |
| Did Not Receive Col. in the past 10 years | 4 (3.6) | 0.679 (.247, 1.863) | .449 | 173 (5.2) |
From the results, it can be seen that there is a relationship between cultural background and ethnicity with colonoscopy screening. Never getting a sigmoidoscopy or colonoscopy test among Marianismo ladies had the most grounded affiliation. The rough chances of never accepting a sigmoidoscopy or colonoscopy test are 2.207 times higher for Marianismo ladies versus Non-Marianismo ladies (95% CI= 1.767, 2.756). A larger number of members announced never getting an FOBT than never accepting a sigmoidoscopy or colonoscopy exam among both Marianismo and Non-Marianismo ladies, separately (82% versus 59% and 74% versus 40%). The chances of not accepting an FOBT in the previous year are 55% lower for Marianismo ladies versus Non-Marianismo ladies (cOR=0.554, 95% CI=0.332, 0.924). This demonstrates the Marianismo develop a defensive factor among Hispanic ladies ages 50 and more established for adherence to CRC screening rules for FOBT.
Discussion
This study provides the main investigation of the impact of cultural background and ethnicity on the colonoscopy screening practices among Hispanic males aged 50 years and above. While bivariate investigations discovered the huge relationship among Marianismo men and CRC screening practices, after altering income levels, age, education and medical coverage scope, Marianismo was not fundamentally connected with any of the CRC screening practices. Nevertheless, remunerations, age, education, medical coverage scope, and children (<18) living in the house were all fundamentally connected with “never got any test,” “not in the know regarding any test,” “never got FOBT,” and “never got sigmoidoscopy or colonoscopy.” The Marianismo males in this examination were found to have fundamentally less wage, less training, less medicinal services scope, and more kids (<18) living in the home than the Non-Marianismo ladies. With those socio-statistic attributes observed to be altogether connected with CRC screening practices, Marianismo and the resultant sociodemographic qualities of the Marianismo males uncovered in this study may add to resultant CRC screening practices as mediators.
With the outcomes from this investigation showing that the socio-statistic attributes delineated by Marianismo males (wage, training, medical coverage, and kids (<18) in the home) could conceivably impact CRC screening conduct in view of revealed socio-statistic results. A closer examination of the potential reasons for these socio-statistic qualities must be analyzed.
In this present investigation, Marianismo males revealed altogether lower salary levels than the Non-Marianismo males and wage was essentially connected with CRC screening practices. This finding fortifies the monetarily defenseless express that the Marianismo-Machismo relationship might cause for Marianismo-displaying men. A male showing the Marianismo trademark may not talk about CRC screening with his spouse any need for colonoscopy screening. Concerning the structure of cathexis, which portrays the social standards encompassing the sexual orientation part that one plays inside a specific culture, Marianismo may cause males showing this attribute to entirely cling to Marianismo paying little respect to its effect on potential wellbeing results in dread of what others may think. The home and offspring of a Marianismo male are his definitive need, and he comes optional.
The study discoveries propose that dialect, cultural background, and to some degree, access to care may clarify colonoscopy screening amongst Hispanics above the age of 50 years. Moreover, it creates the impression that the commitment of every one of these components to CRC screening incongruities changes by national cause among Hispanics. The study was directed utilizing a substantial, broadly illustrative dataset that included adequate quantities of individuals announcing Cuban, Puerto Rican, Mexican, or Dominican birthplace to analyze the wellsprings of CRC screening aberrations in Hispanic subgroups. Hence, these discoveries start to accommodate the clashing after effects of earlier examinations investigating the associates of CRC screening inconsistencies.
Study limitations
The principal limitation of this study is that the information utilized for investigation originated from the interview of 10 interviewers, along these lines, we can’t discover that the announced sociodemographic factors are impacting CRC screening conduct. A longitudinal partner thinks about looking at the impact of the attributes of a Hispanic male showing Marianismo on CRC screening practices is expected to decide the degree of the impact these qualities may have on CRC screening rates among this populace. Another restriction of this examination is that the interview did not make any inquiries with respect to Hispanic subpopulations. There are tremendous contrasts among various Hispanic subgroup impacts CRC screening conduct, however, we can’t examine the distinctions in the present examination. Future CRC screening research including recognizable proof of Hispanic subpopulations might be advantageous in understanding the distinctions inside particular ethnic gatherings.
The size of the sample used in this study for Hispanic males was small, so conclusions for this gathering are speculative. Additionally, the reaction rate for the study is around 65%, and it is along these lines, conceivable that members, especially Hispanics, contrast from their non-member partners. While the course and size of this impact are obscure, and could well shift among Hispanic national inception group, it might prompt under-estimation of the colonoscopy screening amongst Hispanics males of 50 years and above.
Conclusion
This investigation shows that there are numerous different factors to consider as indicators influencing colonoscopy screening among Hispanic males above the age of 50 years, apart from ethnicity and cultural background. Marianismo is a social part showed by individuals from the quickest developing populace in the U.S. As indicated by the U.S Census, starting at July 1, 2012, the Hispanic populace represented 17% of the country’s aggregate populace, and by 2060, this populace is anticipated to represent 31% of the country’s population. Gleaned from this, the social part may act as a hindrance for some Hispanic males as it identifies with looking for deterrent human services. Established researchers misjudge this populace because of social set up that spots them in an auxiliary and docile part which needs to be considered. Marianismo is an under-investigated theme, particularly as it is identified with deterring human services practices in a trademark. A populace depicts it with the most reduced rates of CRC screening. Endeavors outfitted towards understanding social contrasts that may act like obstructions inside a particular ethnic group, similar to the particular Hispanic populace in this study, are urgent in comprehending of what may empower these populaces to look for medical care. Comprehending what may empower a bit of the quick-growing populace with the most reduced rates of colonoscopy screening, will enable us to possibly limit the influence of cultural background and ethnicity on colonoscopy screening among Hispanic men of 50 years and above.
Every year, thousands of people are diagnosed with colorectal cancer. This disease does not discriminate by cultural background, ethnicity, age or sex and therefore from research, it has been found that if detected early, its survival rate is high. The only way to detect this type of cancer is through colonoscopy screening.
Recommendations
The study recommends that research should continue to find other factors influencing colonoscopy screening among the Hispanic males of all ages. Furthermore these group of population should be educated on the benefits of early colonoscopy screening to enhance screening, otherwise this deadly ailment will relentlessly impact on them.
Our Healthcare Writing Help team provides high quality writing services in the field done by healthcare professionals:
– Healthcare Assignment Writing Services
– Healthcare Essay Writing Services
– Healthcare Dissertation Writing Services